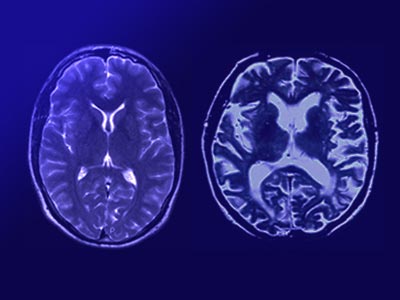
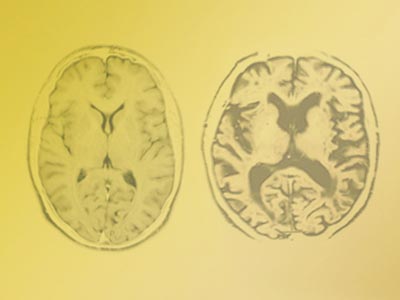
In this conference designed especially for caregivers and lay people, Patricio Reyes discusses the differences between normal aging, dementia, and Alzheimer's disease. He explains the signs and symptoms of Alzheimer's as well as risk factors, diagnosis techniques, disease progression, and treatment options. He also examines the structure of the brain and the function of neurons, which are disrupted by Alzheimer's. Reyes begins his talk with a Jewish blessing for caregivers and throughout the conference recognizes the significant emotional and economic burden Alzheimer's disease imposes on families.
Nuestra misión es la enseñanza y difusión de los principios éticos, jurídicos y económicos de una sociedad de personas libres y responsables.
Universidad Francisco Marroquín