Let me begin by telling you a story, two months ago, I was invited to give a talk in Idaho, that's the northern part of the United States, very cold, a lot of snow.
00:34 |
I grew up in the Philippines so I am scared of snow, and I told my friend "you know, you like snow, so you go and give the lecture in Idaho".
00:47 |
So, he flew to Idaho and when he landed in Idaho, it's a beautiful resort, a skiing resort called n Coeur d'Alene,Idaho. And there was a snow storm, so he went to the auditorium and there was nobody.
01:06 |
So, he was not very happy. So his host said "they will be coming, let's wait for thirty minutes". So he waited for thirty minutes and after thirty minutes, one person came. Son the host said, "Wait for another thirty minutes" and nobody came.
01:28 |
And so, he started giving his talk to one person and he was not very happy, so after thirty minutes he picked up his slides, the computer, and tried to pack up his things, hen wanted to go back to Philadelphia, and the man said, "what are you doing? You cannot do this".
01:47 |
And he said: "No, I am going to leave, right away. They invited me to give a talk and there's only one person." And he said "don't do this to me"; and the speaker said: "no, In will do it". And he said "I told you not to", and he said, why? "because I am the next speaker." So thank you for coming this morning.
02:09 |
What I'd like to discuss with you is the topic that may not be as interesting to many; because it does not involve surgery, it does not involve machines. It involvesn understanding the basic pathology of the human brain, we need to look at the basic mechanisms of life, of cell death.
02:36 |
For instance, I have a saying on my door, in the laboratory, that the reason we know very little about life is because we don't know too much about cell death.
02:51 |
Think about that, if you remember that when you leave this auditorium, that we need to study more about cell death, we will be able to modify and prolong human life with goodn functions. So, I will share with you the thoughts I have.
03:14 |
What is dementia? Dementia refers to medical conditions characterized clinically by progressive decline in intellectual functions, behavior, and activities of dailyn living.
03:28 |
Now, they're usually found in patients who are alert, they're not drowsy, they're not comatose. The symptoms are severe enough to affect the social and/or professionaln life.
03:44 |
As we get older we forget things, but our forgetfulness does not affect our social and professional life, in patients with dementia, it does, because it is progressive.
04:00 |
And generally, dementing illnesses or dementias, affect the late middle age and the older population. Why is that important? Because the World, during the last two decades,n has seen the graying of our population, the fastest growing segment of the population, in the western world, at least, is the older population.
04:26 |
In the United States alone, we expect 20 million older Americans in the next decade. So we have to be prepared to examine patients who suffer from diseases that affect then older population.
04:45 |
So, to make it easy to remember, dementias are characterized by the alphabet, ABC; decline in n Activities of daily living, abnormal n Behavior, and C is n Cognition.
05:04 |
If you remember that, that is the clinical picture of dementia, and that´s why every patient with dementia, we have to assess, in terms of activities of daily living. Are theyn able to drive? Are they able to cook the best recipes? Are they able to shop? particularly for women. If my wife doesn't go to the mall five times a week there is a problem.
05:31 |
Behavior, patients become depressed, they may isolate themselves. So, there may be a depressive component, but underneath that depression is mild problem of memory loss. Andn that is, cognition is the third. So ABC, so whenever you see a patient with dementia assess those three things.
05:59 |
Why is dementia very important? Because in a disease process, wether you have lung disease, you have heart disease, you have kidney disease, if the patient has dementia then cost increases dramatically.
06:18 |
Hospitalization increases, the medications increase in number and compliance may be affected, because the patient forgets and gets confused, so if you have a patient with n heart disease or kidney disease complicated by dementia, management becomes complicated and the cost increases significantly.
06:37 |
For you guys who are beginning, I was a medical student many years ago, so my job as a professor in Medical School was to make things easy for students to remember, that is myn job, so this is n the differential diagnosis that I have written for you, just the word DEMENTIOUS, you use that.
07:01 |
D stands for degenerative disorder, exemplified in Alzheimer's disease and Parkinson's disease. Emotional or psychiatric illness, patients with depression, could tell you theyn forget, but actually they have depression.
07:14 |
Metabolic n or toxic, liver disease, kidney disease, intoxications. Endocrine or thyroid disease, nutritional B12 deficiency, you would be amazed how many older people have low B12, at least inn the United States, where I practice.
07:33 |
Because they don't eat the normal food, you know what they do? They eat sweets. Anybody here has a relative or friend with Alzheimer's disease?
07:41 |
Watch your friend or relative, they like to eat a lot of sweets and that compromises nutrition. Now I'll tell you, I have a long story about that because it gave me a lot ofn opportunity to n work on certain things.
07:59 |
Trauma, Dementia Pugilistica, I happened to be a ring-side physician so I studied the brains of boxers when they died. We have a paper coming up soon on the chronic effects ofn head trauma, secondary effect to boxing.
08:22 |
Infection, immunologic diseases, autoimmune, that is lupus and MS and strokes. So by using the word itself you have the differential diagnosis.
08:31 |
Other groups that you have to distinguish from dementia are cases of encephalopathy or delirium, they are acute processes; dementia is chronic, encephalopathy is acute orn sub-acute.
08:45 |
Dementia is usually not reversible, encephalopathy or delirium is reversible, if you identify the cause early, if you don't they become a dementing process.
08:56 |
Mental retardation, patients, children who are born with this disorder, they are not demented, they´re mentally challenged, we don't usually use the word retardation now, wen use mentally challenged.
09:11 |
Language disorders, facial strokes or brain tumors, they may not be able to speak so they´re aphasic rather than demented. And patients with psychiatric disorders, patientsn with depression will tell you "I cannot remember anything" So how to distinguish that is somehow difficult.
09:30 |
But patients with depression usually, they don't accept effort, they tell you "Dr. Reyes, I don't remember anything" you give them things to do and they say "I cannot don it".
09:42 |
Whereas patients with real memory loss will try very hard, but they still come up short, so this is different. Now as neurologists, these are the common causes of dementia, son we look for 65% of patients, with dementia in adults is due to Alzheimer's disease, recognizing that 35% of these patients may actually have cerobrovascular disease.
10:13 |
Then you have other conditions such as fronto-temporal dementia, Parkinson's disease with dementia, many years ago in Philadelphia, we described the first few cases ofn Alzheimer's disease with Lewy bodies.
10:28 |
These are patients who have progressive dementia with mild parkinsonism. So they were different and when they studied their brains the lesions, the brain showed lesions ofn both Alzheimer's disease and Parkinson's disease.
10:45 |
And you distinguish this because the patients hallucinate, they had visual hallucinations early on and most patients with typical Alzheimer's disease do not have visualn hallucinations early on, and they have parkinsonian symptoms; they´re stiff but they don't shake, they do not have tremors.
11:06 |
So what is Alzheimer's disease? Alzheimer's disease is a form of neurodegeneration and as a teacher in medicine for many years, both in neurology, pathology, psychiatry In think we missed a very important point, many years ago, because now I believe that aging process and degeneration occurs in the womb.
11:32 |
Because once life is formed, degeneration occurs, there is the pruning mechanism, for instance, in embryos, and bad cells die early and good cells are preserved, that´s partn of the aging process, if something happened to the mother, during pregnancy there will be no aging process, so we now have to look at neurodegeneration as a disease that begins many yearsn before.
12:12 |
Because it is not an acute process, it is not a tumor, it is not a stroke, that happens accumulative, it takes many years for degeneration to be symptomatic, it´s liken arthrosclerosis.
12:29 |
You know, if you look at the aorta of men, actually you begin to see plaques during the second decade, so it actually occurs many years before it becomes symptomatic, and thatn is a very important concept to really learn, because when I was in medical school we were not taught that, but I am teaching that every day.
12:59 |
There are now more than five million Americans who have this disease, and I will show you the recent statistics among Hispanic Americans, and it´s become the third mostn expensive disease.
13:16 |
And the caregiver burden, the burden to families is enormous, fifty percent of wives and husbands who take care of patients with Alzheimer's disease, suffer from majorn depression.
13:32 |
And there´s now evidence that caregivers, family members who take care of patients with Alzheimer's disease, also have immunologic problems, because greeving, depression,n prolonged psychiatric symptoms can affect our immune system.
13:52 |
And these are taken from the government, these statistics, and look at the numbers, it's staggering, and if we do not develop a better way of diagnosing and treating thesen patients, we cannot afford to build a nursing home in every corner of the United States.
14:20 |
Economic burden is significant, so this is a major health issue that we are trying to solve in the United States. And this is how it looks in terms of projection, then prevalence of Alzheimer's disease as we get older, increases significantly, at age 85 and beyond the risk for developing Alzheimer´s disease increases to 50%.
14:51 |
The prevalence of Alzheimer's disease in Hispanic population, unfortunately in the United States everybody who speaks Spanish is called Hispanic, so I can pretend I'm Hispanicn because I can carry on a Hispanic conversation, my mother was Hispanic and my father was Chinese, so sometimes I'm Asian and sometimes I'm Hispanic.
15:19 |
That´s how we are categorized or people just ignore us. And look at this, in the year 2050, there is a 600% expected increase in the number of Alzheimer's disease amongn Hispanic population in the United States.
15:40 |
And there are two now main, sort of potential causes for this, one is that type 2 diabetes is very high among Hispanic population and diabetes now is a risk factor forn Alzheimer's disease.
16:00 |
As a matter of fact, I will be part of an investigation that delivers insulin through the nose directly to the brain, and doesn't go through circulation; the other isn hypertension is very high among the Hispanic population in the United States, and cerebrovascular disease is considered also as a risk factor for Alzheimer's disease.
16:31 |
What are the symptoms of Alzheimer's disease? Memory loss is quite often, difficulty for performing familiar tasks, problems with language, and the most common is wordn finding.
16:34 |
You know when we ask for word finding we asked them, What do you call this? This is a watch, but the best way is not only to ask them what this is but what are the parts ofn the watch.
17:01 |
This is the bracelet, how about this one? Now I may have to examine to see how many know the parts What is the name of this one? this is the stem or the winder, what is thisn eyeglasses, anteojos, how about this part? That is the frame or the rim, that is where you pick up the subtle signs of word finding difficulty.
17:29 |
Now, we as neurologists, always ask for the names of the fingers, this is the thumb, the index finger, the middle finger, the ring finger, that is where you put your ring ifn you're married, and the little finger. In Arizona, when I ask patients about that they call this the trigger finger.
17:52 |
In South America, I have been teaching in South America, I have been there many, many times they call this the Roman's finger because that is where they put their marriedn ring, so you have to know the different variations even in the United States. In the East Coast they call this the pinky, not the little finger.
18:20 |
There are also psychiatric symptoms that occur in Alzheimer's disease and the important thing to important to remember that sometimes up to 30% of patients with Alzheimer'sn disease, the behavioral symptoms, psychiatric symptoms precede the cognitive symptoms.
18:39 |
And how do you really begin to suspect this, depression for instance, when it begins at age 50 and beyond, has to be suspected as being secondary, because depression usuallyn begins or schizophrenia begins before that.
19:01 |
So be careful, when you diagnose your patient with depression schizophrenia at age 50 and beyond, underneath that may be a neurologic problem.
19:12 |
The late signs or symptoms are easy to recognize because patients become more forgetful, they're more confused and they now depend on families and relatives for theirn activities of daily living.
19:18 |
Now, you are early in your career, many of you, this is not exciting because, again, you don't do any surgeries, you don't use too many machines, but this to me is the heartn of medicine.
19:47 |
When the patient comes to you or nobody can figure out and the family, all the members of the family are crying in front of you, yet you are only given 15 minutes in then United States to see this patient, how can you practice medicine like that?
20:04 |
If you leave this auditory remembering that medicine must be practiced with total concern, not only for the patient but for the family, not only for the direct health caren issues, but for the emotional component of the disease, we must do that.
20:32 |
How do we evaluate and diagnose patients with Alzheimer's disease or dementia for that matter? We need to go over the medical history, how did this evolve, how did this begin,n and many times, family would say "oh he was fine until a week ago".
20:52 |
There is no such thing as dementia occurring a week ago or Alzheimer's disease, it takes months or even years. So the onset, the beginning is usually ignored as part of then normal aging process and in fact that there is already the beginning of the disease.
21:11 |
I always tell students, and residents, and fellows who work with me, and caregivers, that if I work with my wife, I love my wife very much, if I worked with my wife 24-hours an day every day, I would have acute Alzheimers disease.
21:33 |
And we all do, we all love our spouses, so marriage works because we don't work together 24-hours a day, and that´s why I´m very much against early retirement, that´s whenn people develop heart disease, hypertension.
21:50 |
I have patients, who were fine for many years, and they retire early and they live together, they watch television, their migraine occurred, they said "Dr Reyes, my migrainen is back, my chest is hurting", because you retired early, so there are risks.
22:09 |
How do you asses activities of daily living and behavior? These are just some of the measures we use, because we do research, we helped develop new medications, so we have ton asses all this.
22:26 |
And you see again the ABCs; activities of daily living, behavior, and cognition. So these are the tasks we do to determine whether the patient is improving, stayed the same orn deteriorated.
22:34 |
The many mental state examination, I think you are going to be taught about this and you are going to use this in your clinic; there are thirty points, and what we asses isn orientation, concentration, attention, registration, recent memory, language function, ability to copy and perform tasks, and assess also visual-spatial orientation, we make them draw.
23:10 |
This one here for instance, the intersecting pentagons, and sometimes I ask them to draw a clock and they´re unable to draw a clock, that means that there is a problem withn the visual-spatial orientation.
23:25 |
Now, many years ago, I had a patient from Texas, a very wealthy woman, who every time I saw her would eat two Snicker bars, chocolate bars.
23:38 |
So she had to ask for one minutes of recess to eat two Snicker bars, I never understood the meaning of this, so I went to the medical conference and I asked the faculty,n somebody has to help me explain why all my patients are eating sweets.
24:01 |
Because I asked the dietician to determine whether my patients, who were admitted to the hospital would eat more the dessert, dulce, rather than the main dish, and 100% ofn sweets were eaten first. So those of you who have relatives and friends, let me know whether that´s true or not.
24:25 |
And you know, it´s very hard to test the taste, but a friend of mine from the University of Pennsylvania, told me that we can do the olfactory test, the smell test, becausen 50% of what we taste depends on what we smell, that´s why if you have a runny nose, the flu, you don't taste right.
24:47 |
I didn't know that before, so my grandmother was right, when you misbehave, when I misbehaved when I was a kid, one of the punishments was to pinch the nose and then make youn drink paragoric, it was very bitter.
25:07 |
Because you throw up, in order for you not to throw up, you pinch the nose so you remove the sense of smell, but my mother didn't know there was a relationship, oh myn grandmother didn´t, but by observation.
25:20 |
So what we did was we developed this, University of Pennsylvania Scratch-and-Sniff Test, the sense of smell, the only test available to test our patients with Alzheimer'sn disease, 100% had olfactory deficits, problems with smelling, and now it is being used worldwide.
25:46 |
Unfortunately, the patent went to the University of Pennsylvania, so you guys who will have new observations, remember the institutions that you came from, you can maken contributions to the institutions by using your ideas and developing new tests, and your University will live forever if you do that.
26:16 |
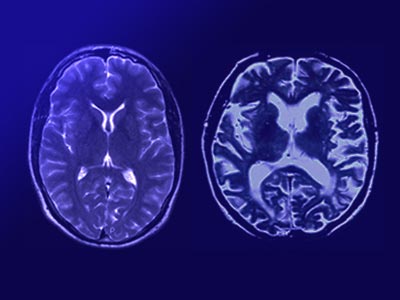
And how about neuro imaging techniques? This is an MRI scan and it doesn't tell us anything except there is atrophy usually, as indicated by this sulci, widened sulci.
26:30 |
This is a PET scan of the brain, showing us that there is very minimal or lack of metabolic activity, in the posterior temporal parietal region, and that´s what you see inn patients who have Alzheimer's disease, this is used mainly for research purposes.
26:52 |
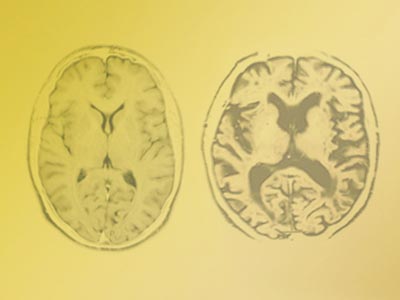
How about neuropathology? Just look at the brain of patients, this is a normal 75-year-old brain, this is a patient with Alzheimer's disease. You can see there is significantn atrophy as evidenced by thinning of the gyri and widening of the sulci.
27:14 |
And in Alzheimer's disease, it affects mainly the structures called the limbic system, and this is what is known as the Papez circuit, in neuro anatomy, remember, Papezn circuit.
27:33 |
And the hippocampus, the mammillary body, cingulate gyrus, the amygdale are all damaged in Alzheimer's disease and these structures govern memory related processes, emotional,n and behavioral expression.
27:53 |
This is my own chemical cast that I used to examine the brain, and this shows senile plaques, which contain central coral amyloid; and these lesions increase in numbers inn Alzheimer's disease, and that´s the reason why most of the reasearch during the last two decades, have focused on what we call the beta amyloid protein, which is the core of the senilen plaque.
28:25 |
It happens that as we age, we also develop plaques, normal people have plaques, the difference is that it is increased in Alzheimer's disease, and under higher magnification,n you can see this is the beta amyloid plaque.
28:42 |
These are degenerative axioms and dendrites telling us that in Alzheimer's disease there´s also lesions affecting the synapses, because without the dendrites and the axioms,n the neurons can no longer communicate, there´s no transmission.
28:58 |
And this is surrounded also by inflammatory cells and that´s why some people believe that inflammation is very important in Alzheimer's disease.
29:11 |
This is the other lesion that develops and this is what we call the neurofibrillary tangles. For many years we just diagnosed them by tests like this one, but we don't known what it was made of, about two decades ago, somebody was able to resolve this.
29:30 |
And now we know that the main protein here is called Tau Protein, TAU, which is a microtubule protein that accumulates in the brain, in the brain cells and then ultimatelyn lead to cell death.
29:44 |
We thought, for many years, that because they accumulate, they kill neurons, now there is evidence that it actually interferes with cell cycle. So, we are evolving in ourn understanding of Alzheimer's disease.
30:03 |
This is again my own way of looking at both, the red is the amyloid plaque; this is amyloid and the green is the neurofibrillary tangle. We like colors, we are Latin so wen like colors, right? and so look at this, it is much better, looks much better, more romantic.
30:30 |
So what are the new therapies? The new therapies are based on what we know now about pathology in the brain, what chemical changes occur, molecular abnormalities that exist,n we learn more about cell death.
30:51 |
How about risk factors? We know there are risk factors, advancing age is one, genetic is another, head trauma, diabetes, hypertension, and now we are looking at heart disease,n particularly a bypass surgery.
31:07 |
And so, we are now able to use new medications, pharmacologic interventions as well as non-pharmacologic, remember, that the symptoms of Alzheimer's disease do not alwaysn require medication, let me tell you an example.
31:31 |
I had a patient, who could not tolerate many medications for sleep, he becomes agitated, you give him something to sleep, he gets worse.
31:43 |
So I made a house call, in the United States you don't do house calls now, but I did, because his a family friend, a very prominent member of our community, a very wealthyn family.
31:57 |
And I asked the wife what was his favorite sport before he got sick. He was an avid golfer, and he had a huge bedroom, we could put my house in their bedroom.
32:17 |
So I said, "why don't we do this, we pretend that we have a putting-green in the bedroom, change the carpet to green, sort of create a little hole there and make him put forn an hour, before he goes to bed".
32:37 |
We never used medication for him, give him a shower after that, he got tired, slept well. So we need to create also different ways of treating behavior, not just dependent onn medications.
32:55 |
Right now we are emphasizing more, at least I do, the importance of lifestyle; nutrition, diet, physical activity, mental activity, socialization, that´s very important in then treatment of patients, with dementia.
33:15 |
So what are the neurochemical changes? There are many, but the most studied is the cholinergic deficiency and there is lack of acetylcholine in the brain, and the severity ofn this chemical deficiency has been related to this variety of dementia.
33:36 |
There is loss of neurons in the nucleus basalis of Meynert, there is diminished acetylcholine level in the cortex and there is a diminished activity of the synthesizing enzymen called acetyltransferase.
33:53 |
There is also evidence that there is an increase in the NMDA activity, which could also result in cell death. And this stimulates the neurons excessively so that the neuronsn are not able to recover and it usually leads to cell death.
34:01 |
So now we have two groups of drugs approved for the treatment of Alzheimer's disease, in the United States; the cholinesterase inhibitors, and the NMDA receptorn antagonist.
34:26 |
I remember many years ago when we first met in Washington DC, sometime in 1985, we had no treatment for Alzheimer's disease, we had no idea what Alzheimer's disease was, andn some of us met in Washington DC, and our mandate n was to develop the first medicine for Alzheimer´s disease,
34:55 |
and who was our president then, in the United States? it was President Reagan, and look at now. In 1993, we help develop the first medicine for Alzheimer´s disease, and thatn was Cognex.
35:10 |
It was not perfect, because 10% can develop chemical hepatitis, but it began the research interest in Alzheimer´s disease, and now we have five.
35:22 |
And last, two years ago, a year-and-a-half ago, we came up with the first skin patch for Alzheimer's disease, because most of these drugs can give you nausea, vomiting,n diarrhea, abdominal cramping, so now we have a skin patch that bypasses the GI system.
35:46 |
So we are getting there and we are working on new drugs, that hopefully will attack the core pathology, rather than just replenish the chemical defficiency, because thesen drugs that we have developed, merely delay the progression, they don't stop the process, they don't revert the process, and this is how it looks.
36:12 |
We have a neuron, presynaptic and postsynaptic, and there is a chemical deficiency there, and there is loss of synapses. And this is something that we learned recently asn well, we were taught in Medical School and in Pharmacology that there is an enzyme called acetylcholinesterase that hydrolyzes acetylcholine.
36:39 |
At least, in the United States I was never taught that there´s such thing as butyl cholinesterase, that also hydrolyses acetylcholine. In Alzheimer´s disease there is evidencen that butyl cholinesterase actually increases.
36:54 |
We have done actual experiments on this and we developed a knock-out mouse where we removed the acetylcholinesterase gene and so it was left with butyl cholinesterase and itn protected the brain. So what are the medicines approved?
37:11 |
Rivastigmine, the first one was Cognex, nobody prescribes that now because of the phatic toxicity. We have Rivastigmine, which is the only cholinesterase inhibitor thatn inhibits both acetylcholinesterase and butyl cholinesterase.
37:28 |
Donepezil or Aricept, only acts on acetylcholinesterase; incidentally Rivastigmine is the only one available in skin patch as well. Galantamine or Razadyne inhibitsn acetylcholinesterase, NMDA receptor antagonist called Memantine or Namenda.
37:51 |
And this is how it´s prescribed in the older times, except for Rivastigmine, which is now a once-a-day patch. The problem with the patch is that 1% may develop skin irritationn because we use latex on it, so you can have skin irritation, in one to two percent, or even allergies. Common side effects are nausea, vomiting, dizziness, vivid dreams, increased urinaryn frequency, hypotension, bradycardia and rhinorrhea.
38:27 |
How about molecular pathology? This is very interesting for us, because you´re really now attacking the core pathology in Alzheimer´s disease. It happens that there aren enzymes called secretases that cleave the beta amyloid protein from the parent molecule called amyloid protein precursor protein, APP.
38:51 |
So imagine that this amyloid protein is hanging from the neuron and if the amyloid is cleaved by beta and gamma secretases, it becomes the nitus or senile plaque. Once we knewn that, we know now that we can develop medications that will inhibit the cleavage of the amyloid protein by those enzymes. The problem right now that we are encountering is some toxicity.
39:29 |
But, I think it´s coming and now it is a great time to get involved with neuroscience because you are just beginning to scratch the surface of the human brain.
39:43 |
And this is how it looks, it is cleaved from the parent molecule. And this is the beta amyloid protein that becomes the senile plaque. I never thought I would ever participaten in these studies when I was like you in medical school.
39:57 |
I hated neurology because it was a figment of my imagination. That´s why I became a brain pathologist in neuropathology because after my training in neurology, I still did notn understand what the brain looked like. I still don't know the human brain, but I´m learning every day.
40:20 |
How about the other pathology, the neurofibrillary tangles? We now know that the Tau protein is the major protein it´s a microtubule associated protein. The difference betweenn the neurofibrillary protein and the normal tau protein is, it is hyperphsophorylated.
40:36 |
So now we know the enzymes that hyperphosphorylate the tau protein and, again, the race is on to develop medications that will prevent hyperphosphorylation, things that wen never thought we could achieve in our lifetime.
40:56 |
This is how it would look in a cartoon, the neurofibrillary protein and the tau protein accumulates and kills neurons.
41:05 |
Risk factors: advancing age genetics, there are two types of genes, so if you ask for genetic testing, make sure, also we are obliged to give genetic counseling to patientsn and their families.
41:20 |
There are two types of genes, the mutational genes, when you have mutations, chromosomes 1, 14, and 21; and also you have the susceptibility gene, it's the ApoE4 the proteinn gene and this carries the cholesterol in our blood.
41:43 |
But if ApoE4 is present, there are three isoforms, ApoE2, ApoE3, and ApoE4; ApoE4 is the one that increases the risk. It doesn't tell us that the patient is going to haven Alzheimer's disease, it simply increases the risk, whereas the mutational genes, if present, almost always guarantees the development of Alzheimers disease before age sixty. Diabetes, we talkn about and traumatic brain injury.,
42:17 |
Vascular pathology, what is vascular dementia? There are different types of dementia that occur in strokes, the large strokes, the small strokes; and many of us in practice,n have seen this white matter lesions in the brain, thre are no real strokes but there are small blood vessels, we call it small vessel ischemic disease and I´ll show you an example.
42:39 |
So vascular dementia, they´re subacute and there is step-wise progression and you look for a focal neurologic deficit, weakness, numbness.
42:51 |
One-sided-gate difficulty, speech difficulty, so there are focal neurological deficits, whereas in Alzheimer's disease you don't see usually focal neurologic deficits.
43:06 |
And this is how it looks sometimes, look at this, this is all due to cerebral vascular disease, patients with hypertensive diabetes. So vascular risk factors hyperlipidemia,n Dr. Alfaro is an expert on this.
43:26 |
Hypertension, diabetes, obesity, that´s another risk-factor that has been attributed to Hispanic Americans, obesity, hypertension, diabetes, smoking history, and alcoholn history. So these are some of the vascular risk-factors, treatment, prevent it.
43:46 |
We can prevent the progression, if we know the causes or reduce the cardiovascular risk factors. In some patients cholinesterase inhibitors may also help, because as I said,n 35% of dementia may be due to mixed cerebral vascular disease and Alzheimer's Disease.
44:04 |
Parkinson´s disease, again, we failed for many decades in teaching that Parkinson's disease can be associated with dementia. We now know that at least a third of patients withn Parkinson´s disease develop progressive dementia.
44:23 |
This is the disease we described in 1986, we called this Alzheimer's disease with Lewy Bodies, the British changed this to Diffused Lewy Body Disease. I still believe that inn our hands many of this represents a subtype of Alzheimer's Disease.
44:43 |
Now, I described the clinical manifestations and the neuropathology of this disease, but they won't publish the paper. I almost changed my name to Smith, because Reyes was notn very nice, but that´s part of academic life.
45:07 |
And do look at this, this is our own laboratory-kind-of-way of looking at Lewy bodies. See that Lewy bodies there, and this is using an antibody, which is very expensive; thisn one is just using fluorescent scope with a chemical, doesn't cause a lot things.
45:27 |
So the clinical manifestation of Alzheimer's disease with Lewy bodies progressive degeneration, there´s memory impairment and there´s also visual hallucination, andn parkinsonism, not Parkinson's disease, but parkinsonism because many times they don't shake, they're stiff, they're slow, and they shuffle. Remember this,
45:48 |
in Parkinson´s disease you have four Ss; they shake, tremors; they´re stiff, S; they´re slow; and they walk like the shuffle, so four Ss. That´s part of my job as an teacher.
46:07 |
Fronto-temporal dementia, they are frequently mistaken as Alzheimer's disease, they´re younger and there are prominent psychiatric symptoms early on, in the later stages itn can look like Alzheimer's disease.
46:24 |
And if you look at the CAT scan or MRI, there is more atrophy in the frontal and temporal region, so we call this fronto-temporal dementia.
46:35 |
Normal pressure hydrocephalus, we have a special program in the United States for patients with NPH, it stands for Normal Pressure Hydrocephalus, now I´m going to show you andn tell you also how I make students remember this.
46:51 |
So Parkinson's disease is four Ss, this is three Ws, okay; they´re whacky, because they forget, they get confused; they are wobbly, because they cannot lift their feet whenn they walk, they march like this; and they´re wet, because they have urinary incontinence, so three Ws. I´m going to quiz your memory, everybody who comes out of this auditorium I´ll ask all then students, okay?
47:23 |
And this is how it looks, look at this, this is frequently mistaken as Alzheimer's disease or Parkinson's disease, because they fall, they shuffle; but this is treatable,n because what we do, we put a shunt and divert the fluid to the peritoneum and the patient recovers.
47:48 |
And these are the psychopharmacologic agents that we use to treat patients with behavioral symptoms, agitation, violence; we use what we call the typical, atypicaln antipsychotic agents.
48:07 |
Unfortunately, this is expensive, so for economic reasons some of us still use Haloperidol; but if money is not an issue we usually use the atypical antipsychotic agents ton avoid the effects causing parkinsonism. And this is just to show you the different, and you can use this in and learn more in neuro pharmacology.
48:39 |
The tenets in prescribing medications begin low and go slow, because patients with dementia and the elderly, do not tolerate the usual doses that we prescribe, so always beginn very slow, with small dosages. There´s no reason to give them 10 mg, if they will do with five mg.
49:01 |
It´s also more economical you let them buy the 10 mg, half the tablet, so they use it for two days, instead of once a day. We, physicians, are being attacked left and right,n particularly in the United States.
49:16 |
We need to think of the economic implications of what we do in our clinic, because our training as I look back, and I have been teaching throughout my life, it has been veryn artificial.
49:30 |
We see them in the hospitals and the clinics, but we don't look into the family structure. We prescribe things and you send them home. Did we ask who lives with you? Did wen examine whether the patient is forgetful or gets confused, will be able to understand and remember what we told them in the clinic.
49:53 |
Do they have money to buy the medications you prescribed, will it affect their economic stability, they´re dependent on welfare, and the mother is the only one working for then family?
50:12 |
So think about that too, as we practice medicine, it´s not just prescription, it´s not ordering tests, let´s look at society as a whole, and I´m sure your founding fathers,n the administration, the dean, the president, and your mentors in this school will be very proud of you if you do that.
50:36 |
Just to show you this, I had a patient from the Midwest who came to see me for Alzheimer's disease, I gave her an experimental drug, a month later she went to Colorado, rentedn a cabin and drew this painting for me.
51:02 |
I have programs for patients, painting classes, reading classes, writing classes, arts, and cooking. And I have made writers of my patients, painters. I have a patient whon held her first art show in Philadelphia after I diagnosed her with Alzheimer's disease.
51:25 |
I had a patient who held her first piano concert after we treated her for Alzheimer's disease. So don't give up, try to understand the process, try to understand the patient,n their families and their impact in society, and always share what you have and be part of your community. Thank you very much.
51:54 |
Audience:Thank you for your talk Dr. Reyes I have two questions, is any new test, biomarker test that you can run before you start getting symptoms? And my second question isn if you can talk about the relation of the early onset of Alzheimer's disease and Down syndrome?
52:23 |
Patricio Reyes:Yes, the first question is biomarker, at present we do not have a single biomarker for Alzheimer's disease, we are working on a labeling compound that we cann inject to people in vivo and we label the amyloid, in the brain.
52:45 |
And this was started in 2004 by a research group from the University of Pittsburg, so it´s called PIB Compound. Unfortunately, it doesn't tell us whether the amyloid is in then blood vessel, in the neuron, or is in the parenchyma, and we still have to wait, whether these patients have Alzheimer disease when they die.
53:08 |
Because Alzheimer's disease is really not a disease, strictly speaking it is a syndrome; you must satisfy neurpoathologic criteria and clinical criteria, because there aren patients that we see at autopsy, and I have been running a brain bank throughout my life, so I get patients from all over the country and outside of the United States sometimes.
53:33 |
And you see these senile plaques, many of them, but when you ask the family and the doctors who took care of the patient, there was no dementia, so you cannot call itn Alzheimer's disease.
53:46 |
Or you can have a patient with dementia, but there are no plaques and tangles and you cannot call that Alzheimer's disease. So these compounds, we hope, will allow us withn time, when we are able to follow up these patients, determine whether the amyloid burden as we see it, will correlate with the clinical manifestations of the disease and will be confirmedn neurpoathologically.
54:13 |
Now, we have studies going on in the cerebral spinal fluid, because what happens's that there are differente types of amyloids, the diffusible amyloid and the non-diffusiblen amyloid, and then we have to look at the ratio between the amyloid level and the tau level.
54:33 |
In Alzheimer's disease, as the disease progresses, the beta amyloid level and the CSF decreases actually, but the tau protein increases. Now, can you use that ratio as an biomarker? That is the question. But to depend on a single biomarker, we don't know, we don't have that right now. Now, we are working on a competitor for the PIB Compound, but it is stilln early on.
55:03 |
The second question is Down syndrome. As you know Down syndrome, and we have an expert on genetics here, is associated with a 21 chromosome mutation, in almost all of them,n when they reach 40 and beyond, they develop cognitive decline, similar to Alzheimer's disease and if you look at the brain, they have lesions of Alzheimer's disease.
55:29 |
And how do you determine this, we talk about mentally retarded or mentally challenged kids, they´re born with, I call it actually, hypomentia, rather than dementia, strictlyn speaking.
55:39 |
Well, what you do with patients who are born, mentally challenged kids, you do a neuropsychological testing, early on in life, should you have a baseline, and they remain liken that for about 30 years to 40 years, and after that they decline.
56:04 |
Now you call it dementia, because they have achieved a certain level of cognitive function and now it is declining, and that´s when you consider Alzheimer's disease
56:18 |
And unfortunately ,they´re very hard to treat as well. I have one patient who saw me last Monday, whose cousin told me that he's doing very well with one of the cholinesterasen inhibitors, but it is an anecdote, but nobody has really shown me any very good response to any treatment, at present.
56:38 |
Audience:Muchas graciasfor this wonderful conference, I noticed that you didn´t mention MCI, and if you see a patient with amnestic MCI would you treat him with cholinesterase inhibitors?
56:54 |
Patricio Reyes:Thank you very much, everybody heard the question, MCI? Remember that this is not ATandT but MCI, it stands for mild cognitive impairment, and MCI went bankrupt,n ATandT is up.
57:12 |
And these are patients who come to us and consult us, and they live in the community, many of them. They work, but they come to us and say "Dr. Reyes I´m not the same, I´mn forgetting, I have to write more now, and sometimes I get confused with directions, but I am able to go to work". Now, our challenge is how to diagnose Alzheimer's disease as early asn possible.
57:40 |
So these patients may fall into the category of mild cognitive impairment, you cannot call it dementia because they are able to work, they are able to socialize, so they'ren not demented, they are impaired, cognitively; not to the point of being demented, then we categorize them into different subtypes.
58:05 |
We have patients who have MCI, have difficulty following commands only, like executive functions, like I would ask a patient, try to imagine I´m visiting you and you´ren offering me a glass of wine, so you open up the bottle, you get a glass and you pour it an offer it, hopefully with the right hand, not alone the left hand, that is executive function, that´sn frontal lobe.
58:34 |
That´s a different connotation, because Alzheimer's disease, as I mentioned to you, affects more the temporal lobe and the limbic system; whereas if a patient has problemsn exclusively with remembering things, that is the amnestic type and that has a very high correlation with conversion to Alzheimer's disease.
59:03 |
MCI patients have 11 to 15% chance or risk of converting to Alzheimer's disease every year; and the amnestic type has the highest conversion rate. The other type that we lookn for is what we call visual-spatial; difficulty assessing the relationship between objects and space, and that can also be associated with memory loss or could be alone.
59:34 |
Now there is this subtype of Alzheimer's disease that we have reported, patients who come to us with problem with vision, so these patients drive ophthalmologists crazy,n because they´re perfect, their memory is good but they have problems with visual orientation.
59:58 |
They have problems driving, they have problems with the doors, opening the doors, but they don't see double and that´s what we call the posterior variant of Alzheimer'sn disease, because if you look at them clinically, they have more problems with visual-spatial orientation, and the atrophy begins more in the parietal lobe rather than the temporal lobe.
01:00:27 |
Now when it comes to treatment, I always tell patients that there´s no treatment for MCI, approved by the FDA, but at least 50% of them, they like to take one of then cholinesterase inhibitors, hoping that one of these agents will delay the progression of the symptom.
01:00:46 |
Now, I always tell them, because I have been working with the department of agriculture, my friend from the U.S. Department of Agriculture, we are finding out that certainn fruits and vegetables are very good for the brain.
01:01:01 |
So, I always include in my treatment vegetables and fruits for the brain, and I advise them to take fruits and vegetables with colors, because the American diet is bland;n cheeseburger, hamburger, there´s no color in it.
01:01:20 |
So you have to add color, spinach, green leaves vegetables, blueberries, blackberries, all the berries, avocado; if you want nuts, walnuts, almonds, and we are working veryn hard because these are cheap, although blueberries are not in the United States.
01:01:47 |
Once we release those data, the handful will cost ; everybody takes advantage of even the scientific data, because we believe that they have high antioxidant properties,n that protects the brain.
01:02:02 |
Audience:Dr Reyes, you mentioned President Reagan, we all admire his communication skills, could you, if you can or if it´s possible, give us your idea of why it was so fastn his deterioration, because after he gave his speech, as he was living the presidency, which was a brilliant speech, eight months later he was with severe Alzheimer's. What could have happenedn there?
01:02:32 |
Patricio Reyes:This is something, that´s a very good question, the question is the patient was doing well and eight months later he could not recognize his wife.
01:02:43 |
It´s not a very uncommon complaint, what happens probably is that there are mild symptoms that occur, but it´s very hard for late people, and even, with due respect,n primary care doctors.
01:03:00 |
Even my colleagues in neurology, you are not trained to really assess behavior cognition, and activities of daily living; they are not included, we are not taught that,n even now there is very little teaching in that, even in the American setting.
01:03:19 |
So those symptoms are relegated as part of the aging process, normal process, and then something happens, boom. The most common cause of exacerbation of symptoms that leadsn to hospitalization, at least in the United States, is urinary track infection.
01:03:39 |
A patient who has mild symptoms develops any form of metabolic or infectious process, symptoms just blossom, increase significantly. Another thing that can cause what´sn seemingly is a very rapid progression is stress.
01:04:04 |
Many patients would only show symptoms after, say, the death of a spouse, the death of a son, and that´s when they begin to appreciate that there´s a problem.
01:04:22 |
Then, another one is, another illness, now remember now, patients with dementia, as I told you, are middle-aged and older population, so many of them have comorbid othern medical conditions, they have hypertension, heart disease, kidney, liver, lung problems.
01:04:42 |
So any of these concomitant medications, hypertension, that exacerbate, could also enhance the dementing process, it becomes clinically apparent, and that is many timesn what happens.
01:05:01 |
Even minor head trauma can exacerbate the symptoms rapidly, so I think, in many situations at least, there´s probably already, and you see this after surgery.
01:05:17 |
I have a patient who was 56 years of age, a very wealthy man, they just removed a disk, suposedly no symptoms at all, and after the disk surgery he developed very rapidlyn progressive dementia.
01:05:35 |
And we looked at him from head to foot and there was nothing, now there's a different connotation with that. You need to exclude in a rapidly progressive dementia, threen months, six months, look for this, because if the patient is doing like this that is PRIAM Disease or Mad Cow Disease, unless proven otherwise.
01:05:57 |
Toxins can do that, so you look for toxins, you look for what we call Carcinomatous meningitis, can do that. So we have an obligation to exclude outer conditions, but oncen we´ve excluded those, chances are the patient has a very slowly progressive dementing process.
01:06:16 |
Audience:I have a question about using hormone replacement therapy, isn't it supposed, like you said before, in the beginning of the presentation, that if you know how then cells are killed that you can develop better...
01:06:43 |
Patricio Reyes:Okay, let me just move on here... the question is hormone therapy?
01:06:51 |
Audience:Yes, because supposedly hormone therapy is to maintain you young and everything, but they have found that hormone replacement therapy increases dementia risk, so it'sn contradicting, if you are trying to maintain youthfulness but...
01:07:10 |
Patricio Reyes:Very good, okay, I got your point, I got your question. Well, the question is, as you know in the life cycle of women, there´s natural menopause that occurs andn estrogen is not produced anymore to a large quality and hormone replacement therapy after menopause, could it prevent Alzheimer's disease?
01:07:40 |
This is just to show an experiment, many years ago, the one on the left is a neuron that was cultured without estrogen, this one was cultured with estrogen, and look at then number of dendrites here and axioms, there are many.
01:08:07 |
So this is with estrogen, this is without; so we believe that after this experiment that estrogen may be important in regenerating neurons, but we have done some clinicaln studies as well, in patients who have Alzheimer's disease after menopause and estrogen replacement therapy did not improve them.
01:08:35 |
We, however believe, that women who had their ovaries and uterus removed early on in life, will benefit from hormone replacement therapy but not after the development ofn Alzheimer's disease or after menopause, we don't know that.
01:08:59 |
And, also there are certain risks with hormone therapy after menopause, there is DBD increase maybe, and there is the risk for female genital track cancer, for instance.n Some cases, some investigators think it´s over rated, but there´s some who believe that it is real. The question is after menopause does it help patients?
01:09:28 |
We don't know the answer, there is evidence now that it may actually increase the incidence of Alzheimer's disease after menopause. The other question is: is syntheticn estrogen different from naturally occuring estrogen or estrogen plus progesterone? So, unfortunately we don't have those answers at present time, we used to recommend estrogen therapy but nown we don't, because of the lack of evidence.
00:01 |
Initial credits
00:20 |
Opening remarks
02:09 |
Study of cell death
03:13.800000000000011 |
What is dementia?
Dementia in older people
Characteristics
Activities of daily living
Behavior and cognition
Why is dementia important?
Differential diagnosis of dementia
D-E-M-E-N-T-I-A-S
Differential diagnoses of other diseases
Encephalopathy or delirium
Mental retardation or mentally challenged kids
Language disorders
Psychiatric disorders
Common causes of dementia
Alzheimer's disease
Cerebrovascular disease
Frontotemporal dementia
Parkinson's disease
Lewy bodies
11:07 |
What is Alzheimer's disease?
Aging process and neurodegeneration
Atherosclerosis example
Number of Americans with the disease
Caregiver burden
Prevalence of Alzheimer's in Hispanic population
Type 2 diabetes
Hypertension
Cerebrovascular disease
16:30 |
What are the symptoms of Alzheimer's?
Memory loss
Difficulty performing familiar tasks
Problems with language
Word finding
Psychiatric symptoms
Depression
Late signs
The heart of medicine
20:33 |
How do doctors evaluate and diagnose patients?
Early retirement
Assessment instruments
Mini-mental state evaluation (MMSE)
Problems with smell and taste
Olfactory testing
University of Pennsylvania scratch-and-sniff Alzheimer's test
Neuroimaging techniques
Neuropathology
Limbic system
Neuritic plaques (NPs)
Neurofibrillary tangles (NFTs)
30:30.5 |
What are the new therapies?
New treatments for dementia
Medication not always required
Importance of a healthy lifestyle
Neurochemical changes
Approved drugs for the treatment of Alzheimer's
Cognex, first medication for Alzheimer's, 1993
Development of skin patches
Neuron function
Normal cholinergic function
Approved medicines
Cholinesterase inhibitors (ChEls)
NMDA receptor antagonist
Cholinesterase inhibitors prescription
Common side effects
Molecular pathology
Neuritic plaque pathology
Neurofibrillary tangle pathology
41:05 |
Risk factors
Genetics
Vascular dementia
Vascular risk factors
Treatment and prevention
44:2.5 |
Other dementias
Parkinson's disease and dementia
Alzheimer's disease with Lewy bodies
Frontotemporal dementia
Normal pressure hydrocephalus
Psychopharmacologic agents
49:09 |
Medicine and society
50:38 |
Final words
51:54 |
Question and answer period
Is there any biomarker test you can run before getting dementia symptoms? Can you talk about the relationship between the early onset of Alzheimer's and Down syndrome?
Biomarker for Alzheimer's
Pittsburgh Compound B
Cerebrospinal fluid
Alzheimer's and Down syndrome
Are patients with amnestic type mild cognitive impairment (MCI) treated with cholinesterase inhibitors?
Executive function type
Amnestic type
Visuospatial type
Vision problems type
No approved treatment for MCI
Colorful fruits and vegetables
Why did Alzheimer's deteriorate President Ronald Reagan so fast?
Mild symptoms
Urinary tract infection (UTI)
Stress
Another illness
Early detection
Why does hormone replacement therapy (HRT) increase the risk for dementia?
Alzheimer’s Disease and Related Dementias: Diagnosis and Treatment
|
04 de febrero de 2009 |
Vistas: 449
In this conference at Universidad Francisco Marroquín School of Medicine, Patricio Reyes discusses Alzheimer's disease and related dementias; focusing on symptoms, the latest diagnosis techniques and treatment therapies. He comments on how encephalopathy and delirium differ from Alzheimer's and describes frontotemporal dementia, normal pressure hydrocephalus, and other forms of dementia. He also explains the risk factors for Alzheimer's and dementia, including heredity, lifestyle, and other medical conditions including diabetes and Parkinson's disease. According to Reyes, the incidence of Alzheimer's among Hispanics in the United States is increasingly prevalent due to several factors. Finally, he offers advice to future physicians on what to keep in mind when treating patients and the role of medicine in today's society.