So what I decided to do in your announcement, the topic was Past, Present, and Future, I just gave this talk to the faculty in Arizona most recently, so In thought that this would be more pertinent.
00:40 |
Although, we can discuss what we used to do, and what we are doing, and what we are going to use to treat patients, to diagnose and treat patients withn Alzheimer's disease in the future.
00:52 |
Now, we are talking about a disease that was actually discovered many years ago, more than a century ago. And this was the first patient, who was taken caren of by Dr. Alois Alzheimer, he was a German neuropathologist.
01:10 |
And believe it or not, Auguste was a 52-year-old woman when she died; she had epilepsy and became demented. And when Dr. Alois Alzheimer studied the brain hen found an increased numbers of neuritic plaques or senile plaques and neurofibrillary tangles.
01:34 |
Not too long ago, we actually celebrated, the world celebrated the centennial of Alzheimer's disease, and had this done in Germany, where he was born, and asn you can see here, he died at a young age; age 51, he was a psychiatrist at that time.
01:56 |
Psychiatrists, there were no neurologists just psychiatrists, and actually, many of them were also neuropathologists, and that influenced my personal medicaln career; so, I didn't learn too much about the brain when I finished neurology, so I did neuropathology and general pathology.
02:19 |
As a matter of fact, the first chairman of psychiatry at John Hopkin's University was a neuropatholigist. That's how powerful neuropathology was in the oldenn times.
02:32 |
So, in the beginning of the 20th century this was described and the autopsy was done in 1906. It was only Kraepelin, in 1910, who proposed that this diseasen should be called Alzheimer's disease.
02:50 |
But strictly speaking, it is actually a syndrome and not a disease; because in a syndrome you have two components that you must satisfy and that is then clinical characteristics and the neuropathological characteristics, both of them must be present.
03:07 |
So, if you have plaques and tangles in the brain and the patient is not demented you cannot call that Alzheimer's disease; or vice versa, if you have an patient with progressive dementia and there are no plaques and tangles you cannot call that Alzheimer's disease; so, both have to be present.
03:25 |
So what is Alzheimer's disease? It is a neurodegenerative disorder, it's now the seventh leading cause of death in the United Sates, that counts for about 65n to 70% of patients with dementia.
03:39 |
It affects the middle aged and elderly; 10% of patients of individual 65 years and older are expected to have Alzheimer's disease. And 40 to 50% of patientsn 85 years and above, are expected to have Alzheimer's disease; and more than 5 million Americans suffer from this disease right now.
04:04 |
And as a pathologist, as I review medical records for instance; many pathologists do not put Alzheimer's disease as the primary cause of death.
04:15 |
Because they don't die from Alzheimer's they die from pneumonia, from sepsis; so, many times, since this is based on autopsy records, it is actuallyn underdiagnosed or underestimated.
04:26 |
And this disease is also difficult, in the sense that you end up treating the entire family. And more and more, at least in the United States, we aren expected to see more patients, every 15 to 20 minutes, every 30 minutes, but if you see patients with memory loss, with behavioral symptoms, with family members crying, how can you dismissn those patients?
04:57 |
You have to give a very comprehensive medical history, you have to examine the patients physically, neurologically, behaviorally, and then give them yourn diagnosis, the workup and council the patients.
05:11 |
It involves the entire family many times and the caregiver burden is tremendous, because many times these patients require 24-hour care, unless they are inn nursing homes, the family members suffer, they have to provide the care at home.
05:31 |
And so, now we have evidence that 50% of caregivers suffer from major depression, they have to be treated. And now there is new evidence that significantn number of caregivers suffer from immunologic disorders, there is no question that prolonged, for instance, depression, stress can affect the immune system.
06:00 |
This is just to show you a small percentage of Alzheimer's disease, probably 5%, may have what is known as familial ,and it is usually autosomal dominant,n and the onset of disease is usually before age sixty-five, so if you have patients suffering from the disease usually before age sixty, one should consider the possibility of Familialn Alzheimer's disease.
06:32 |
In terms of differential diagnosis this I what I do for medical students and residents, who work with me and fellows. And this is sort of the differentialn diagnosis that I want them to remember, whenever they´re confronted with a patient with any type of dementia or Alzheimer's disease.
06:54 |
And just to use the word "dementias" and you will cover many of the disease processes that can cause dementia or mimic Alzheimer's disease.
07:04 |
So more and more, and actually I´m preaching every day now, this concept of the triangle of life, that we are governed, our lives are affected by what wen inherited, for instance, from our parents, the genetic, the environment and lifestyle. But in patients with dementia there are three things that we have to evaluate.
07:36 |
That is activities of daily living, are they able to carry out their activities or daily living regularly, how about behavior, up to 30% of patients withn Alzheimer's disease will present with depression, irritability, anxiety, before cognitive symptoms are recognized.
07:58 |
So, it is very important that if a middle-aged patient presents with new symptoms of depression, of psychiatric symptoms, that we look at them carefully,n because underneath that there may be a dementing process and then we worry about cognition.
08:20 |
For many years, we taught in schools; and I'm guilty of this, when we say dementia or Alzheimer's disease, we only refer to memory loss and cognition andn that is wrong, because we have now evidence that patients may actually get lost first, before they complain of memory loss.
08:41 |
Patients may suffer from depression first before they are found to have memory loss, so these other symptoms can precede the development of cognitiven symptoms.
08:53 |
So what are the early signs of dementia and memory loss? Difficulties with familiar tasks, some patients of ours are referred to us because they are involvedn in accidents.
09:06 |
For many years their driving record was impeccable, and all of a sudden in three months, they have three tickets or violations. Be careful with changes inn their activities or daily living.
09:21 |
Why all of a sudden in three months they have three police tickets, was it because they were violating traffic rules or they were victims of a disease? Andn that has tremendous implications.
09:39 |
When I was in training at the University of Miami, I did general pathology and neuropathology, if you go to Miami Beach and many of you have been to Miamin Beach, the average age of patients at that time was 76-years-old, I happened to be part of the medical examiner´s team as part of my training.
09:57 |
So we would get older people being hit by cars in Miami Beach, and I began to question my mentors because they were victims of accidents, and I said, aren they really victims of accidents or are they victims of disease? And my mentor grabed my lips and said you are opening a can of worms; because it has tremendous implications.
10:27 |
You know, if they´re victims of disease, then the insurance carrier will be different, and the driver will be absolved of crime, because it was actually then fault of the patient, can you imagine that? Yet, we were not allowed to discuss the subject, and now, because I´m no longer in training, I can discuss this.
10:59 |
Impaired judgment, problem with abstract thinking. I have been asked many times, people who sell assets, businesses, they found out that the owner of then businesses who sold the businesses were actually impaired, cognitively.
11:22 |
Was it a legal sale or not? So, we have to make decisions whether the sale was legal or not, was it appropriate or not, or was the patient taken advantagen of, even by their own relatives, making them sign contracts.
11:43 |
So, part of my job is to protect my patients' rights, for instance, and this is changing our role as physicians, at least in the United States. Missplacingn objects, I have a patient who lost three cars in three months, because she forgot where she parked her car.
12:09 |
So, it has tremendous impact on the economics as well, changes in mood and behavior. So these are symptoms that may not be impressive in terms of cognitiven functions, but if you look at the cause of the symptoms, because most of them are behavioral, mood changes, all of a sudden, mom and dad, or grandma or grandpa has become irritable, what is then reason for this?
12:38 |
They´re not sleeping right and they deny symptoms; they don't want to socialize anymore, they want just to watch television. So, beware of behavioraln symptoms that begin at later life, because many psychiatric diseases, as a rule, begin early on in life, not at age fifty or sixty.
13:06 |
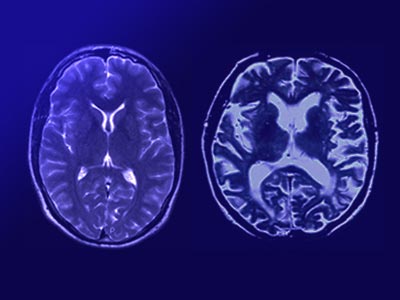
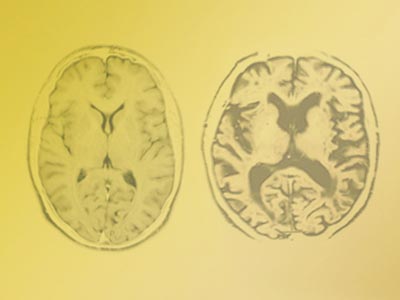
This is just to show us the differences that you see or the abnormalities, rather, that you look for in patients who have Alzheimer's disease.
13:23 |
Using a PET scan here on the right and you can see hypometabolism, red is good, because that means that there´s good metabolism; and here, in the postn temporal and parietal region, there´s almost nonexistent, and that´s what you see in patients with Alzheimer's disease.
13:40 |
The MRI simply tells us that there is diffuse cerebral atrophy, and if you see atrophy, mainly in the frontal lobe and temporal lobe, that may ben representative of another disease called frontotemporal dementia.
13:54 |
And this type of dementing illness, FTD for short, they have more behavioral symptoms rather than cognitive symptoms early on and that is a differentn pathologic or clinical entity.
14:11 |
And this is just to show us what happens in the brain, this is the normal seventy-five year-old and then there´s this patient who is seventy-five years oldn with atrophy.
14:24 |
And in Alzheimer's disease, looking at the normal structure, the hippocampus is a target structure and you can see here, you cut the brain like this and then normal individual has a beautiful hippocampus, and here you have lost the hippocampus.
14:46 |
And you can see that with a CAT scan or MRI through the ventricular dilatation of the temporal horn.
14:54 |
So what happens in the brain, there is atrophy, there are increased number of senile plaques, increased number of neurofibrillary tangles, and loss ofn synapses.
15:08 |
These are the plaques and tangles, these are neurofibrillary tangles, and these are neuritic plaques, senile plaques; and this is what happens, these are then pathological hallmarks of Alzheimer's disease.
15:22 |
At Barrow Neurologic Institute we have developed a new way of looking at this, using fluorescent technique, we show that the green fluorescent structuren here, represents neurofibrillary tangles and the red represents the senile plaque.
15:44 |
Here are examples of neurofibrillary tangles, and we now know that is made up from a protein called tau, T-A-U, and this tau protein in Alzheimer's diseasen is different from normal individuals because they are hyperphosphorylated.
16:07 |
So, with that information and we know now what are the enzymes that hyperphosphorilate this, so we can now develop new agents to preventn hyperphosphorylation. And this is again, under fluorescent technique you can see how beautiful this is.
16:31 |
Tau protein, as I mentioned, is the main component of neurofibrillary tangles, it is a microtubule-associated protein, that is important in transportingn nutrients, to and from the cell body of neurons.
16:48 |
So, if it accumulates in neurons then the transport of nutrients is impeded, and also it does affect now on cell cycles, so it can kill neurons.
17:05 |
The senile plaque however, is the major focus of research worldwide, and that´s because it contains the amyloid protein, we call now beta-amyloid, and then senile plaque is made up of the central core of beta-amyloid, surrounded by degenerated axons and dendrites and inflammatory cells; and I'll show you this, just to show you, those senilen plaques that occurr.
17:42 |
And my own technique, this is my own, so you won't see this in another slide, because this is only available in my laboratory; look at this beautifuln beta-amyloid protein surrounded by degenerated axons and dendrites.
17:58 |
And around this also are inflammatory cells and that´s why in some studies some investigators have claimed that anti-inflammatory agents could help patientsn with Alzheimer's disease.
18:15 |
In controlled studies however, supported by the NIH and the National Institute of Aging, the study using anti-inflammatory cells, like iboprufen, has failedn to show any benefits in patients with Alzheimer's disease.
18:33 |
Let's move on now to senile plaque and just to show you how we isolate, using our technique, the beta-amyloid. It was actually this gentleman here, Georgen Glenner, who isolated the amyloid, and it was not too long ago.
18:54 |
Unfortunately, he is not with us and he passed, and this was his original paper, The Congophilic Microangiopathy,meaning there is a disease calledn congophilic angiopathy, it means that amyloid is deposited in the blood vessels, and that weakens the walls and it causes intracerebral hemorrhages.
19:20 |
And they are usually polar hemorrhages, so if you see a patient with intracerebral hemorrhages, usually in polar distribution and the patient doesn't haven cerebral vascular risk factors, no hypertension, no heart disease, think of congophilic angiopathy.
19:42 |
So, Glenner and Wong, isolated and purified amyloid protein from cerebral vessels and that really began the study of beta-amyloid, and look at thisn Alzheimer's disease and Down syndrome, because many patients with Down syndrome at age forty and beyond, develop symptoms of Alzheimer's disease and if you examine the brain, they also haven large numbers of senile plaques and neurofibrillary tangles.
20:16 |
So now we know that the amyloid core in the plaque is about thirty-nine to fifty-three amino acid molecule. That's cleaved from a parent molecule called APP,n and these are cleaved or it is cleaved by secretases.
20:38 |
And if the amyloid protein is cleaved by beta and gamma secretase, they give rise to an amyloid protein that becomes the core of the senile plaque, and nown we have identified patients who have mutations of APP, amyloid precursor protein.
21:01 |
And, if the mutation is present, and usually three genes are involved, three chromosomes; chromosome 1, 14, and 21; in Down syndrome it is almost guaranteed,n I didn't say always, that those individuals will develop Alzheimer's disease early on in life.
21:26 |
So, right now as we speak, there are now current investigations using or trying the efficacy and safety of secretases in Alzheimer's disease patients. One ofn the problems we have to contempt with are side effects of these agents, at least the first generation of secretases may have some toxicity with them.
21:51 |
And this is a cartoon to show you how the beta-amyloid, as I mentioned to you this is the APP protein, the parent molecule, hanging from the wall of then neuron, and look at this is cleaved by two enzymes, beta secretase and gamma secretase, and that becomes the senile plaque.
22:18 |
Because everybody was wondering where the plaques came from, even one investigator here, said it came from cysts of Borrelia Burgdorferi, this is the agentn that causes Lyme disease, so everybody had his own hypothesis before this was confirmed, this is just for historical kind of interest.
22:46 |
So because of these, we now have potential new therapies for Alzheimers disease; beta secretase inhibitors, gamma secretase inhibitors, we can also stimulaten A beta-lowering agents immunotherapy, I'll discuss that later, anti-aggregation agents.
23:08 |
Increase clearance of A beta and alpha secretase agonist, meaning you promote alpha secretase so that there's less A beta.
23:18 |
In Phoenix, we are doing what we call the EPIX study, it is an alpha-secretase agonist, a new compound, a novel compound, it has antihistamine effects, itn increases acetylcholine production which is, because in Alzheimer's disease there is acetylcholine deficiency, and we have evidence that this agent, I cannot give you the name itself, it isn numbered, it prevents beta-amyloid formation.
23:52 |
So now we are attacking, not just the symptoms or the deficiency, but we are attacking the core problem in this disease. Then we have what is known as then amyloid labeling compound and this started at the University of Pittsburg, it´s called the Pittsburg Compound.
24:13 |
What it does is, the patient is injected with radioactive material and it labels the amyloid protein in the brain, and you scan the brain, you do a PET scan,n you will see the amyloid finding.
24:28 |
So you can now, with this compound they hope to measure the amount of amyloid in the brain, even before the symptoms are manifested. Now the problem is thatn Alzheimer's disease without symptoms?
24:46 |
Are you diagnosing patients prematurely? And there are a lot of implications when you write the diagnosis of Alzheimer's disease; patients may not be hiredn anymore to work, insurance companies may not insure them anymore; or raise the premium significantly, so it´s very difficult to make a definitive diagnosis based on just a clinical orn diagnostic study.
25:20 |
We also have another study, that is actually a competition of the Pittsburg Compound, we think it is a better drug because it has a longer lifespan, and youn can do regional and detailed studies.
25:38 |
The Pittsburg Compound only is, you can only measure it in a few minutes, it leaves the brain after a few minutes, this one stays for about twenty minutes,n so you can do more regional studies and may provide early diagnosis in patients associated with amyloid disorders.
26:03 |
And that may also be used to verify if the treatment you are giving is affecting the disease by the amount of amyloid labeling that is present. So we aren moving very rapidly in this, very exciting era to be in neuroscience.
26:23 |
And I hope our medical students here will be able to recruit some. And this is how it looks in a cartoon, you inject the patient radioactive material and youn scan the brain and you can see this amyloid labeling.
26:40 |
Something I never thought I would be part of when I was in medical school, so we have a few medical students, I think I will bring them with me ton Phoenix.
26:56 |
So then, let's go back to bedside, when I was in the University of Texas, I was an assistant professor to one of the more wealthiest families in Texas, an woman with Alzheimer's disease; and every time I saw here in the clinic, she asked for a one-minute break, she had to eat two chocolate bars, two chocolate bars.
27:25 |
So then I asked our dietician to do a little research for me, every time she saw a patient come in to the hospital, and I was the attending, I wanted her ton know whether the patient ate the main dish first or finished the main dish first or the dessert, dulce. One hundred percent dessert first, ice-cream, pudding, flan, tacos no.
27:58 |
So, in the ground rounds of the University of Texas, I remember now, this was my first job, and my first job was to head the department. So, I was very youngn when I headed the department, I said, somebody has to help me, I don't know why my patients are eating a lot of sweets, and the dean was sitting there, and nobody could answer my question.
28:25 |
And the Dean said that any faculty member who was seen eating sweets in the cafeteria had to see Dr. Reyes. So, I became the subject of jokes there, in Sann Antonio, and in Texas if you are not 6 foot 5, you don't wear a ten gallon hat you don't count as much.
28:46 |
And I don't have any of those. So two years later, I was recruited by Jefferson's Medical School in Philadelphia, it´s one of the oldest medical schools bornn in 1824, so when I was made the head of the laboratory and the Alzheimer's Disease Center, I established.
29:10 |
And I met a friend from the University of Pennsylvania, and I told him I had this problem, I cannot explain why my patients are eating a lot of sweets.
29:20 |
And he said I have the laboratory, you have the patients, you can use my laboratory. And it happens that 50% of what we taste depends on what we smell.
29:30 |
So I started seeing my patients there, testing them, and 100 %,all the patients with Alzheimer's disease have problems with olfaction, have smelln problems.
29:47 |
You cannot use this in advanced cases, in mild to moderate stages of Alzheimer's, 100%. So we appeared in Good Morning America, all those talk shows, wen became, we worked with different perfume companies because you have to smell.
30:07 |
If you use a perfume that nobody can smell it doesn't work. Now, we became consultants to fire department; you cannot be a fireman if you can't smelln smoke.
30:18 |
We don't realize how much smell is important professionally and socially, giving medications, nutritional supplements; because it affects taste; if you don'tn smell right then 50% of your taste is also affected.
30:41 |
And there are people who claim they have lost the sense of smell at work, so there is workermen compensation cases, so we have to determine who isn malingering, who has a real olfactory deficiency.
30:59 |
So, now we have the University of Pennsylvania´s scratch-and-sniff test. It´s being used now not only for Alzheimer's disease, but for MS, and as a predictorn for Parkinson's disease.
31:12 |
And this started from one bedside observation, a patient who was eating lots of sweets. So you don't have to be a molecular biologist, you can be a goodn clinician and be observant, and you can make good contributions.
31:25 |
And this is, sort of taken from an article we published, because nobody would believe us. Remember now, this was happening in the late eighties, mid-to-laten eighties, and if you, in the United States, if your name is Reyes, you may not count that much compared to if your name is Smith.
32:01 |
So, I had, actually, to draw the anatomy, all of us went to medical school, what did they teach us about the olfactory system in man? I used to round withn Dr. Carpenter, who wrote the text book of Neuroanatomy, he used to come to the University of Miami every winter, and in his book there is very little about the olfactory system.
32:30 |
So I had to convince the medical community that there is a problem in the olfactory system, I had to sort of draw the anatomy, the human anatomy, of then olfactory system based on subhuman primates anatomy, mostly in monkeys and in small mammals.
32:57 |
And this is how it looked. See it was published in the archives of neurology, and what I did too was, if you look this is the olfactory bulb and track comingn through the nose.
33:11 |
And look at the connections, all of these, this is dorsomedial nucleus, prepiriform cortex, intracranial cortex, hippocampus, hypothalamus, basal nucleus,n all parts of the limbic system. And that´s what is affected mostly in Alzheimer's disease, the limbic system.
33:37 |
What I did too, is every part of this, I took a section of patients with Alzheimer's disease and counted the number of plaques and tangles in all of thesen and compared this with other parts of the brain, and believe it or not, these have the highest density of plaques and tangles, the connections of the human olfactory system.
34:05 |
So, I was able to convince now, so it was finally published and this is sort of the quantitative measures that we did to prove that the neurofibrillaryn tangles and senile plaques are highest in certain parts of the olfactory system.
34:28 |
And we also doubled it up with clinical tests, we tried 40 types of odors, in increasing and decreasing concentrations and we proved that patients withn Alzheimer's disease have significant olfactory deficits, so we did it both, clinically and pathologically.
34:51 |
And this is what came out; unfortunately, the patent is with the University of Pennsylvania. And this is how it looks, you give a patient something ton scratch, you scratch this and the smell comes out, and you give them choices, so many of them miss the right order, and because of this we became the headlines of different dailies in then United States.
35:27 |
And look at this one in New Jersey, claiming that nosing is the first sign of Alzheimer's disease. We never said that, but that´s an interpretation of then press.
35:42 |
Now, how about the biochemical and neurochemical changes? For beginners, this is just to show us a small area in the brain, and look at this, this is veryn small this is called the nucleus basalis of Meynert.
36:02 |
In studying neurologic diseases, you really don't have to lose many neurons, like in Parkinson's disease, it begins with a small area called sustancia negra,n and if those neurons are lost, patients develop Parkinson's disease.
36:22 |
And everyone of us here knows what Parkinson´s disease does to all patients, and you actually lose only very few cells.
36:29 |
Same thing in Alzheimer's disease, the process begins here, the cells here produce acetylcholine, and if the cells die, then the cerebral cortex, then hippocampus, are all deprived of acetylcholine. The level of acetylcholine deficiency correlates with the level of dementia.
36:56 |
And that´s why after this was done the race was on to develop the first medicine, and we helped develop the first medicine for Alzheimer's disease. We workedn on it from 1986 and in 1993, the first U.S. FDA approved treatment happened in the United States, and that was Cognex.
37:23 |
Those of us who have been in practice for a while use Cognex, but the problem was that 10% of patients who took Cognex, developed hepatitis, chemicaln hepatitis.
37:35 |
So, it was not the best drug, but it was a great beginning, because before that there was nothing to offer. And there was no interest in treating orn diagnosing Alzheimer's disease during my time, our doctoral in Alzheimer's disease was Diagnose Adiós.
37:57 |
Nothing to offer, nobody wants to see you, psychiatrists tell us it is a neurologic problem because they have behavioral problems; we say,send them back ton psychiatry.
38:11 |
And the internist said this was a purely brain problem. So nobody wanted them, can you imagine that? You looked at 5 million Americans that nobody wanted ton treat.
38:24 |
If we did not have this progression, we did not advance, and now we have five medications approved; and just a year-and-a-half ago we came up with the firstn skin patch for Alzheimer's disease.
38:39 |
No longer tablets or capsules, a skin patch once a day, bypassing the gastrointestinal system, which is usually the side effect in any of the cholinesterasen inhibitors. And this was the first medicine that we helped develop.
38:59 |
It´s called Tacrine, the brand name was Cognex, and nobody uses this now because we have better drugs. It was actually first tested by Dr. Summers fromn California, a psychiatrist who unfortunately, was criticized for charging patients, there was some ethical issue about the way he gave this to some patients; but nevertheless we showed that inn some patients it was effective.
39:32 |
And this is how it went in 1993, Cognex, the Japanese counterpart removed the liver toxicity and came up with Aricept. This is a Novartis product,n Rivastigmine, and this is the only cholinesterase inhibitors that inhibits both, acetylcholinesterase and butyrylcholinesterase and this is what we used to develop the skin patch.
40:00 |
So, Rivastigmine is the only medication that has a skin patch, the rest are tablets. This last medication here, is an NMDA receptor antagonist; NMDAn receptors are important because they stimulates neurons, to excite neurons.
40:23 |
But if you excite neurons excessively you´ll also kill the neurons, because the neurons have to rest, they can only sustain stimulation to a certain point,n so this drug supposedly antagonizes excessive stimulation, that's why this one can be used in combination with any of these drugs, because their actions are different.
40:51 |
These four were designed to replenish correct the chemical deficiency, this one is to antagonize excessive neuronal excitation.
41:02 |
Now, we are working on this, we call an orphan drug. An orphan drug is one that was developed in someplace and nobody wanted to use it anymore.
41:17 |
And this was a Russian drug, and a company from California stumbled upon this, it actually uses antiallergy, antihistamine; but they found out that it has,n actually a lot of effects, good effects; it increases acetylcholine, it has serotonin effects, and it has also effects on amyloid formation.
41:38 |
So, we now use this experimentally only, it´s not available to the public yet, in addition to Aricept, and I can tell you most of our patients are quiten happy, without knowing, because this is a double blind study.
42:04 |
But at least looking at patients clinically, many of them have not deteriorated, and the patients and their families are quite happy. Whether we can verifyn that scientifically or not, I don´t know; but I think that in a year or two, we should be able to see the results of this study.
42:29 |
We also developed animal models; one of the problems in Alzheimer´s disease for many decades is that we don't have animals that we can try medicationsn on.
42:41 |
This is an animal model, for instance, where we knock out the gene that causes acetylcholinesterase, because the question is, if you remove acetyln cholinesterase, the animal for instance, will have a lot of acetylcholine, and if you have excess acetylcholine the muscles get weak and you get paralyzed also.
43:06 |
And that´s what nerve gas does, so we stumbled upon this too. So now you can actually use this as a model for nerve gas, which is very important in certainn countries right now.
43:24 |
Now, we also did this because there was a question on whether there is one enzyme, acetylcholinesterase or butyrylcholinesterase, so in Alzheimer´s diseasen as we talked, there is death of neurons that produce acetylcholine and also there is acetylcholinesterase that's present that hydrolyses acetylcholine, so whatever is remaining it stilln hydrolyses acetylcholinesterase.
43:53 |
In Alzheimer's disease, there´s another enzyme that increases and that is butyrylcholinesterase. So when we remove, for instance the acetylcholinesterase,n animals die because of paralysis and the muscles are abnormal, whereas the brain will look normal.
44:15 |
Ergo, there´s something else that´s doing the hydrolysis of acetylcholine and that is butyrylcholinesterase. And this just came out in 2007 and we provedn that using histopathological and neurochemical techniques, that mice without cholinesterase, the brain is normal because the butyrylcholinesterase takes over the functions, but the muscles aren not normal because there is no butyrylcholinesterase in the muscles.
44:58 |
How about genetics? Whenever we do genetic studies in patients with Alzheimer´s disease, we must remember that there are two type of genes, the mutationaln genes and the risk-factor genes.
45:12 |
If there is mutation of these chromosomes, again as I alluded to previously, patients will develop or are bound to develop Alzheimer's disease early on,n before age sixty or sixty-five.
45:27 |
The risk-factor gene, like ApoE4 does not guarantee the development of Alzheimer's disease, it merely increases the risk, if you have the gene. And this genen occurs more in patients who have late onset Alzheimer's disease.
45:48 |
Late onset Alzheimer's disease implies that the disease begins after age sixty-five, whereas early onset begins before age sixty-five. And this gene, then gene product is 299 amino acid proteins.
46:09 |
They transport like a protein and incidentally the gene is found in chromosome 19, and so there is a relationship also between this gene product andn cholesterol.
46:23 |
If you look at patients with Alzheimer's disease many of them have elevated cholesterol. This tells us what cells produce ApoE, and we now believe that ApoE,n for instance, has a lot of role in say inflammation, immuno regulation, and regeneration.
46:50 |
For instance, if one has intracerebral hemorrhages and the patient has ApoE4, allele or gene, chance for recovery is much lower, neurologic recovery is muchn lower, if the gene is present.
47:08 |
So it´s one predictor of neurologic recovery after intracerebral hemorrhage. Also we are studying its effects or relationship with head trauma, traumaticn brain injury for instance, if the patient has a traumatic brain injury and ApoE4 early on.
47:27 |
The question is, does it affect recovery as well, and that is being done too in heart disease.
47:35 |
These are the current statistics, 40 to 65% of Alzheimer's disease patients have at least one copy of the ApoE4 allele. One third of Alzheimer's diseasen patients are ApoE4 negative, and there are also exceptions.
48:02 |
Even if the patient has two copies, some patients may never develop Alzheimer's disease, so when you give genetic counseling, it doesn't mean that then patient has ApoE4 allele, that the patient has Alzheimer's disease, it merely increases.
48:19 |
It has been concluded that one copy of the gene increases the risk by up to three-and-a-half times the normal population, whereas two copies may increase then risk to eight times.
48:33 |
So that´s how we distinguish the mutational genes from the risk-factor gene. And just to recapitulate what I said, the ApoE gene is found in chromosomen 19.
48:51 |
And there are three types: ApoE2, ApoE3, and ApoE4. And look at this, the ApoE2 is linked to type 3 hyperlipoproteinemia and there´s conflicting evidencen that it may increase or decrease arthrosclerosis.
49:07 |
But ApoE4 has been now implicated in Alzheimers' disease, arthrosclerosis, and decreased neurite growth, meaning regeneration is impeded if ApoE4 isn present.
49:24 |
And this is the distribution, the percentage of individuals with ApoE isoform. ApoE3 is much more common, the most common, and ApoE2 is as common asn ApoE4.
49:43 |
But the combination of ApoE4 and ApoE3 is about 25%. Now we talk about nonpharmacologic approaches to Alzheimer's disease, there´s increasing evidence thatn lifestyle, we also have a role in the treatment or even prevention of Alzheimer's disease.
50:14 |
Now friends of mine have done some great studies, using mice, for instance, if a group of mice are given or are fed every other day, and the other group isn fed everyday, the ones that are fed every other day live longer and are smarter.
50:35 |
So caloric restriction is important in some cases and these are the evidence so far today, that caloric restriction is important in humans.
50:57 |
Look at this, Dr. Mattson and I were together at the University of Kentucky, he is now the head of the Metabolic Unit of the National Institute of Aging, andn his experiments as early as 2003, intermittent fasting delay symptom onset and lifespan of Huntington's disease mice.
51:18 |
We have an animal model for Huntingtons disease, because in neurodegenerative disorders like Parkinson's disease, Alzheimer's disease, ALS and Huntington'sn disease, the basic mechanism may have an overlap.
51:33 |
The lesions may be different but some basic pathogenic factors may overlap. So this is very important, this is the newest, again by my friend Mattson, thatn alternate caloric restriction improves clinical findings in overweight adult asthmatics.
51:53 |
And these are the theories on caloric restriction and why they increase longevity, mitohormesis, I will not discuss this but it happens that in some cases,n for instance, the hippocampal neurons, which are the ones that are important in memory and behavior, they would need some amount of hunger to stimulate the production of certain proteins thatn are important for regeneration, for memory.
52:28 |
One of the, sort of suspected proteins is the hitch high protein, so when there is hunger and less, for instance, glucose to a certain level, we don't known that level, may stimulate the production of proteins that are important for neuronal survivor.
52:50 |
DHA, insluin signaling, for instance now there´s evidence that low insulin in the brain may be harmful for neurons, and so some friends of mine have asked men to help develop an intranasal insulin that goes directly to the brain, doesn´t join the circulation, and increases the amount of insulin available to brain cells.
53:21 |
And there's the initial evidence is that patients improve significantly, so we are going to do larger studies using intranasal insulin.
53:32 |
Free radical, we all know can be destructive, neurons need free radicals but if it´s excessive they kill neurons. Glycation, and also we have what is knownn as transgenic mouse model.
53:48 |
Transgenic mice are very important because we can study now animals, we can make the animals produce plaques and tangles, because we know the genes, what ton inject in these animals.
54:04 |
Like in these animals for instance, we tweaked; we changed three genes, so they develop all the lesions of Alzheimer's disease. So we can try medicationsn early on and if it works, then we can try it in humans.
54:21 |
Before that we didn't have the opportunity to do this. And so, while we were working on animals, I also am preaching things like the importance of genes,n lifestyle, and environment. And to me this is very important as we study human brain function.
54:49 |
I have in our program physical and mental exercises, we emphasize the importance of nutrition; fruits and vegetables with high antioxidant properties,n omega-3 fatty acids, for instance.
55:09 |
Because before we do that, we have tried this on animals, and it´s amazing because old animals are like humans, older couples; and brain cells are like oldern couples, the older the neurons are they don't talk to each other anymore, they live together, but they don't talk to each other, they are like married couples, and so our job is to make themn talk again.
55:41 |
And that´s what we are doing, so we have all kinds of exercises, water exercises, we try to look at every patient, what they liked to do, when they weren younger, I have art classes, painting, music, writing, I now have two patients who are writing books for kids.
56:00 |
They never knew they could write. I have a patient who had his first art show, after he was diagnosed with Alzheimers disease. I had a patient who had hern first piano concert, the wife of a lawyer, after she was diagnosed with Alzheimer's disease.
56:17 |
So there are many things that we can do that will not require drugs. I had a patient for instance, I was called before I left, because a prominent member ofn the family was getting worse in a nursing home, and all the medicines they gave her got her worse, so I went to the nursing home and investigated.
56:41 |
This woman would get very violent, very mean at about 3:30, so everybody said, that it was sun downing, a lot of patients with dementia or any neurologicn disease, they get worse in the afternoon during sundown or before sundown, why we don't know.
57:07 |
So with sundowning what we can do is give them a little bit of a typical antipsychotic, about thirty minutes, an hour, before sundown. And that is veryn important for young doctors, when you prescribe psychopharmacologic agents; make sure that you know when the symptoms begin, because you cannot say three times a day, like most people do.
57:34 |
But if the symptoms occur about 4 o'clock, you dont want to give it at 1 o'clock, because by that time the amount of medicine may not be sufficient.
57:48 |
So when I talked to the patient, and you know why she becomes very agitated at 3:30? Because she hates black people, and the nursing aid who takes care ofn her is black. Well that is not the problem of the patient, we need to investigate first, and the patient does not need medication.
58:18 |
I have another patient, who also would do the same thing and the only reason he would become violent or irritable, was because at sundown or before sundown,n when the sun hits the west side there´s a shadow in his room, and he would be scared of the shadow, he would imagine that it was a person, because they become paranoid.
58:48 |
That doesn't need medication, you remove the shadow, so there are many things that we can do without using medication that will help patients.
59:01 |
So, in the future the basic research is critical, the challenge is how to apply the research data to diagnosis and therapy, and we need to understand then mechanisms that lead to the development Alzheimer's disease.
59:19 |
We must now ask ourselves what is the molecular basis of cognition, how does the brain adapt to age-related changes, how much cognitive reserve isn there?
59:33 |
There's evidence that those of us who went to school, and all of us here went to school we're good, have much more reserve, and that delays Alzheimer'sn disease versus if you didn't go to school, so education is protective.
59:52 |
As a matter of fact, I had the opportunity to examine a Supreme Court Justice Judge in Philadelphia, and we gave him the hardest test we could imagine and hen came out with flying colors.
01:00:09 |
The reason is that he was a brilliant man, he was a graduate of Harvard Law School, with all the medals you could imagine, and if you give him the testn that we give to everyone he would pass it, because his IQ was so high, so even if he lost twenty points, he was still above average.
01:00:30 |
Because the tests that we give are for average individuals, whereas if you are just making it and you lose five points you are marked as abnormal.
01:00:40 |
We have a neuropsychologist here tonight and I hope you can validate that, the neuropsychologic test that we use are for average individuals, not for highn achievers, so when you use those measures make sure that you correlate that with the educational level or the IQ level, because, and what the question was, what should we do now Dr. Reyes?
01:01:05 |
His colleages said, "Dr. Reyes, he´s no longer the same judge and he´s making decisions about human lives everyday", so you are put in this path.
01:01:18 |
I never figured that I would be in this position in medical schoo,l so what I did was, I told him that he needs to have a leave of absence for six months,n six months for retest the patient.
01:01:35 |
Because in dementia, one of the criterion is that you must show progression of symptoms; in six months we retested him and there was some progression ofn symptoms.
01:01:45 |
So then I was able to say, I suggest or I recommend early retirement. Because I was able to show, based on repeated neuropsychological tests, that theren was a significant decline and that´s what we have to do.
01:02:02 |
A lot of money is being spent on beta-amyloid research, as a matter of fact, before I left, I had a national interview on the use of this beta secretasesn and how to develop, and what is my opinion on the use of this in terms of and efficacy of this and toxicity.
01:02:26 |
Synapses are also targets, this refers to beta amyloid diffusible ligands, which become the nidus for senile plaque. And look at this, this is a newn protein that has been identified, it´s like hemoglobin, but it´s present in the brain, particulary in the hippocampus.
01:02:48 |
So this will be a subject of investigation as well, immunization, and we'll talk about this.
01:02:56 |
The first attempt to immunize a patient was to inject two types of active immunization, where you inject patients with protein and the patient developsn antibodies. The problem was this compound resulted in 6% of encephalitis, so it was stopped completely.
01:03:21 |
A new method has been developed that´s called passive immunization, so the antibody is raised in say test tubes and it is produced outside the human bodyn and the antibody is injected.
01:03:38 |
And that may be effective, the other one is partial fragments of the amyloid protein will be the one injected. The patient still develops antibodies butn the complications are much less, but that is all in preparation.
01:04:00 |
Tau protein also is subject of investigation that´s the future; they have now identified a mutant tau in frontotemporal dementia and Parkinson'sn disease.
01:04:12 |
And this is the latest finding, that the tau protein may cause alteration of the cell cycle and lead to cell death, and they can trigger cell death,n particularly if they´re in the early stages of the disease and they form soluble forms.
01:04:31 |
If you remove the tau gene, in animals, there´s no behavioral abnormality in those animals, in spite of large amounts of senile plaques. So, these twon lesions are the subjects of intense investigations.
01:04:54 |
There is also now evidence that certain diseases, I mentioned to you ALS, Lewy body dementia, frontotemporal dementia, Parkinson's disease, Huntington'sn disease, and Creutzfeldt-Jacob disease, may have a common denominator in certain cases.
01:05:13 |
I can show you as a neuropathologist that in some cases, I see Lewy bodies that you see in Parkinson's disease, as well as plaques and tangles in the samen neuron, because the brain cell can only there act finite change, so you cannot diagnose a case based on one lesion, because it can only change so many times.
01:05:38 |
So these are all degenerative conditions and it is very important to recognize that there may be some common changes and occur abnormalities.
01:05:53 |
We are also now learning more about the normal aging process and what causes cell death. Oxidative distress can be deleterious depending on the amount ofn reactive protein, of reactive species.
01:06:13 |
Some investigators now have isolated the gene that controls lifespan, so whether that will be important in Alzheimer's disease we don't know.n Inflammation, some investigators have shown that tumor necrosis factor may be present in Alzheimer's disease and could kill cells.
01:06:39 |
Not as the primary cause but the secondary phenomena, that's why if we ever use an anti- inflammatory agents it should be a secondary kind of agent,n rather than the primary agent,
01:06:54 |
on over production of free radicals that lead to cell death. Then we have new insights, something we´ve been told for many years in medical school andn postgraduate training, that there is no regeneration in the brain, that is no longer true.
01:07:15 |
Look at this, in the hippocampus in particular, new cells have formed. There´s even evidence that the new cells that have formed are better than the oldern ones.
01:07:30 |
They´re able to adapt and they are more excitable, too much exaltation however, we don't want them to be too excited. And this may be importantn information processing in forming new memories. But it can also be impeded or decreased by stress; it´s amazing what stress can do.
01:07:56 |
So, future treatment of Alzheimer's disease will depend on the investigations we´re doing in beta-amyloid and tau, and the relationship betweenn Alzheimer's disease and other neurodegenerative conditions, the relationship between normal aging and Alzheimer's disease.
01:08:15 |
I mentioned this morning in my lecture for the medical students that in my office I have this saying or quotation, I have done this from day one, when In became an attending, that: The reason why we know very little about life, is because we do not know much about cell death.
01:08:41 |
Because if we know cell death, what causes cell death we can modify life, we can prolong life, improve function of life, and that´s what we´re doing, alln of these are focused on what kills cells.
01:08:56 |
And these are new insights; the other thing that we are going to be challenged is when we talk about neurologic disease, unlike other organs, the neuronsn survive in a cellular muleau.
01:09:16 |
Neurons don't survive alone, they have glial cells that support them, they have microglial and endothelial, so doing experiments in test tubes usingn neuronal cultures is in the past, may not be ideal.
01:09:35 |
But that´s very artificial, that´s very good at looking at tumors for instance or looking at a specific process, but in a diseased condition, particularlyn in neurodegenerative disorders that may not be applicable, and we have to think that neurons don't exist in the brain alone they depend on other cells, and they work together.
01:09:57 |
So these are just some of the things that we´re doing at Barrow Neurological Institute, what we have involved in the treatment, understanding, diagnosticn studies, we are looking at the relationship between dementia an Alzheimer's disease on one hand, and CABG surgery for instance.
01:10:23 |
We are involved in vaccine production and we are involved with animal studies as well, so I´m very excited. So, for some of your medical students, I hopen that I will hear from them, that by coming, it got them interested in neuroscience.
01:10:45 |
Okay, and this is just the institutions we work with and I thank you very much for your coming here.
01:10:58 |
Audience:Would you comment on the other side of the spectrum, how low should we, cardiologists or doctors, decrease cholesterol in human beings, because In think there have been certain observations about behavioral changes with excessive lower in our cholesterol and I don't find the answer anywhere.
01:11:21 |
Dr. Reyes:Our principle is to decrease the cholesterol as low as possible, because there´s evidence that cholesterol also causes inflammation in then brain.
01:11:38 |
And as a matter of fact, symvastatin or one of the statins is being used for the treatment of not only of Alzheimer's disease, but for MS, to diminishn inflammation, because MS has tremendous amounts of inflammatory response.
01:11:57 |
So, I always emphasize the need to lower cholesterol levels, because 35% of our patients with Alzheimer's disease have cerebral vascular disease as well.n So that alone is an important observation to consider.
01:12:15 |
Audience:I have a question, I didn't understand very much when you were talking about mitochondrial... when you were talking about caloricn restriction.
01:12:24 |
Dr. Reyes:That´s what I was talking about, that brain cells need a little bit of low or a little bit of "hunger", but we don't know that level yet. Andn that´s actually a very difficult hypothesis to support.
01:12:43 |
But, there´s a speculation that in neurodegenerative disorders there´s a lack of substrate, for instance like glucose, to stimulate neurons to producen proteins that are important, for regeneration or survival.
01:13:02 |
Audience:I remember that several years ago, in several meetings, people said that education was so important that countries in Africa would have a lot ofn Alzheimer's disease, but over the years, I don't think that nowadays everybody thinks the same way, because although they may have a larger frequency or prevalence of disease, it is not as badn as you may think.
01:13:32 |
And now I wonder if the lack of excessive food in those countries may help them into not develop as frequently dementia as we used to think this was goingn to happen. Do you think this is possible?
01:13:51 |
Dr. Reyes:You want me to answer now? Yes, I think, first of all, the lifespan in Africa is much shorter than the western world. It´s like smoking, theyn say that smoking prevents Parkinsons disease; the problem is they don't develop Parkinson's disease because they die of lung cancer early on.
01:14:11 |
So they don't, nobody develops Parkinson's if you smoke two packs a day, okay. But in Africa, and I... there was a report about that, in three countriesn actually, China and India, and so we´re looking at the Mediterranean diet, the Indian diet, curry and its effects.
01:14:33 |
In China, I've been there four times, there is a lot of Alzheimer's disease; their criteria however are different from us. There they just get a history,n you may not have a CAT scan, you have Alzheimer's disease and you cannot do that in the United States.
01:14:50 |
There´s no autopsy verification, the data that we present can verify the autopsy that´s why many of us have brain banks, perhaps University of Franciscon Marroquín can have the first brain bank in Central America, how is that?
01:15:10 |
And so you have to decide when you want to get involved because this becomes a major health problem for all countries.
01:15:20 |
So, nutrition is very important, as we saidl I think I mentioned earlier today that in India, where I've been, I was a visiting professor, the diet isn very important, the lifespan also, is shorter, they have less Alzheimer's disease, and is it related to diet or caloric restriction, as the economic status in India is different from ourn economic status here.
01:15:55 |
A friend told me that Indians in India, not in the United States, who are overweight belong to the upper class, so that is the effect of westernization, In guess; so potentially diet and caloric intake may also affect the incidents of Alzheimer's disease .
01:16:23 |
And thirdly, the gene, the ApoE4 allele, Chinese claim that they have less or studies have shown rather, that ApoE4 is much less common in Chinese,n particularly in those who live in Hong Kong, so that is another risk-factor that we need to consider.
01:16:49 |
Audience:I have another question, now that I can see all the information that you have, do you think that there is any difference between this threen medications that we use as inhibitors for the cholinestaerase, is any different, is any better than the other one?
01:17:11 |
And I say this because, you see, we are bombarded by these pharmaceutical companies and then, actually you don't know, some are more expensive than then others, and you have to make a choice sometimes and of course we like to use the best medicine available. Do you think there is any difference or you don't think so?
01:17:32 |
Dr. Reyes:I think they are very similar, I only use Rivastigmine more often because I believe in the dual action. The problem with Rivastigmine before wasn the capsule form causes quite a bit of nausea, vomiting and diarrhea, so they call you in the middle of the night, that the patient is throwing up in the emergency room, and you want to sleepn too.
01:17:57 |
But now that we have the patch, we have almost eliminated that side effect. Now, my rule is to tell the patients we have three cholinesterase inhibitors.n Now there is a question with the Razadyne, there is a question of unexplained death.
01:18:21 |
We don't know why there was an increase in death in the Razadyne population treated. Aricept is the easiest to prescribe, you give them, the incidents ofn diarrhea, nausea, vomiting is very low.
01:18:35 |
But Aricept has a very long half-life, seventy-two hours. So if your patient has side effects they will stay for seventy-two hours. And if your patientsn needs general surgery that requires general anesthesia, it will be there. So, whereas Razadyne or Galantamine and Rivastigmine, their half-life is about eight hours, Rivastigmine will ben longer, about ten hours. So the side effects will not last that long.
01:19:11 |
So, we still have problems with any of these, as a class, the cholinesterase inhibitors can lead to gastrointestinal symptoms, they can have cardiacn effects, they can cause bradichardia, because they´re cholinergic agents, so in patients with cardiac arrhythmia or unstable angina or recent MI, we don't want to give it to them, they cann cause hypotension.
01:19:42 |
Now this one is very interesting to me because two days ago I got a call from the University of Pennsylvania, a collegue of mine said: "Pat my patient whon was taking Aricept, had always a soar throat".
01:20:00 |
And I said, why don´t you do this, you stop the Aricept and tell me, call me. He called me two days later and he said the soar throat had disappeared. Youn know why? Because there is an increased nasal secretion and he was having post nasal drip.
01:20:27 |
That´s cholinesterase inhibitors side effect, increased urination frequency; many of our patients, men and women have problems going to the bathroom atn night, it´s one of the common problems.
01:20:39 |
So I warn them, if I give you this medicine you may go to the bathroom more often because that is, again, a cholinergic effect.
01:20:50 |
Aricept is noted for vivid dreaming. Very few ask about that question, but if you ask patients who are taking any of these agents, particularly Aricept,n many of them complain, Dr. I´m dreaming a lot. Sometimes they wake up, violent sometimes. I had a patient not too long ago, who dreamt he was in a cage with a tiger after going to the zoo, son there's a risk going to the zoo if you´re taking one of these agents.
01:21:24 |
And so he woke up fighting the tiger, imagine that, so I stopped the Aricept. And what you can do now is, although they have similar actions they are notn all the same, so because of the advent of these other drugs, the different cholinesterases, I rotate them.
01:21:42 |
So many of my patients would, well 50% of them, would like to be started on Rivastigmine and 50% would be on Aricept, we rarely use Galantamine.
01:22:00 |
But when they start to decline, say six to twelve months later, I shift them, and there's evidence that those patients who did not respond or begin ton decline with Aricept after six to twelve months, they do better with Rivastigmine.
01:22:18 |
And those who have side effects due to Aricept may do better when you shift them to Rivastigmine. And we do that all the time on the hypertensiven medications, and we have migraine patients, we do that in MS, we rotate them.
01:22:35 |
So we do the same thing now, in Parkinson's disease also it´s very important because the only approved drug for dementia in Parkinson´s disease, becausen at least one third of patients with Parkinson´s disease develop dementia, and we didn't teach that, we failed to teach that before, now we know that and the only approved treatment at least inn the United States is Rivastigmine.
01:22:56 |
Audience:I ask that question because we have more experience with Rivastigmine and I think that, I don't know why, I think it is a matter of marketing andn so on, but you worry sometimes about using a medication that is available everywhere and so on.
01:23:13 |
I was involved in the patch study, it was obvious, it was double blind but you could tell who was taking it because of the side effects; and actuall,y youn could tell that the medicine was working, they really got better, and of course without the side effects.
01:23:31 |
And last question, you know it is interesting, research is very important everywhere and we need to do more research here in Guatemala. Do you think thatn there is any possibility that, we neurologists, could be involved in one of those studies that you're doing in Barrows?
01:23:53 |
Dr. Reyes:Oh, absolutely, absolutely. When I was Consultant for the National Institute of Aging for 14 years, that´s why I traveled all over the world,n because we fostered collaboration.
01:24:06 |
But you don't need the National Institute of Health, if you want we can work together, we do, I work together with different institutions, the Universityn of Indiana, I have collaboration with other institutions around the world, and it is a matter of organization and giving a commitment, because this is a commitment.
01:24:31 |
It's right when I started the brain bank program in the United States; I sort of pioneered that brain bank, rapid brain autopsy, because when I wasn training, I criticized my training.
01:24:46 |
The reason is pathologists are trained to... is there a pathologist here? I'm safe. But what we do in pathology is if a patient dies and there's ann autopsy, we do the organs, we remove the body, and dump it in formol.
01:25:07 |
Then if we remember after three months there´s a body there, that´s been autopsed, the organs, we examine, we confirm the diagnosis. Is there a stroke, isn there a heart attack or whatever.
01:25:18 |
But that is only confirmatory, it doesn't allow us to advance in the understanding of the disease. So when I finished my training I wrote a paper and In wrote a grant to the United States National Institute of Health saying, "we need to examine the brain fresh because after death the proteins disappear, the chemicals, the receptors change", andn that´s why we did not advance for centuries, for many years.
01:25:55 |
And I was called Dr. Frankenstein, I got all different names, and they said, "I don't know where he came from, he didn't go to school here, that kind ofn things; he's trying to do this, and he's too ambitious..."
01:26:08 |
I mean we get this pink slip, where you write... I get all these personal criticism, nothing to do with what I wrote, everything was personal, that I wasn neurologist trying to do nonhuman things; and so my patients in Texas supported my research.
01:26:29 |
And that´s what I think is very important for us, if you do a good job and you really produce something, people in the community will support you, I didn that in San Antonio, I did that in Philadelphia, and I am doing that in Phoenix.
01:26:49 |
The community responds, but you have to be credible, you have to produce, you have to remain focused on that, and you have to deliver what youn promised.
01:26:58 |
But the community will respond. There are many people there whose hearts and minds need stimulation, (...) just an example; I´m able to come here becausen of what? A friend of mine from Guatemala, who introduced me to Dr. Alfaro, the Marroquín, and told me that "we would like you to come".
01:27:27 |
If they were not happy with what they saw at Barrow, they wouldn´t be able to do that. And I can name you different patients outside and within the Unitedn States, who are willing to support what we have done and what we do. And so I hope this will just be the beginning of this effort and I will do everything I can.
01:27:59 |
We should never forget that we are successful because of the community that supported us, we owe our success many times, to the people who supported us inn our community.
01:28:15 |
So, whenever we succeed we must never turn our backs on the community that made us successful, we must share it with them, we must go out with them, andn learn from them because we owe our success, many times, to the people who live in our community.
01:28:36 |
And to me, your school here is unique, because I was told that they never accept governmental money, tax money, you preach human rights, freedom, socialn justice, and I read a book written by your founder about this, something that I'd never seen in other medical school in the world.
01:29:02 |
But I think it´s very important, we need this in every medical school in the world, and if we do this, everybody will have no problem with healthcare.n Thank you very much.
00:01 |
Initial credits
00:20 |
Introduction
00:54 |
History of Alzheimer's disease
First patient
Alois Alzheimer's biography
Emil Kraepelin's proposal, 1910
Characteristics of a syndrome
03:26.5 |
Alzheimer's disease
Statistics
Underestimation
Impact on families and caregivers
Familial Alzheimer's
06:34 |
Differential diagnosis
Medical conditions that can mimic Alzheimer's
Key symptoms
Activities of daily living
Behavior
Cognition
08:55 |
Early signs of dementia
Difficulty with familiar tasks
Victims of disease
Impaired judgment and problems with abstract thinking
Misplacing objects
Changes in mood and behavior
Denial of symptoms
13:08 |
Physical symptoms
Neuroimaging features
PET scan
MRI
Healthy brain versus brain atrophy
Hipppocampus
Neuropathology
Pathological hallmarks
Neurofibrillary tangles
Tau protein
Senile plaques
Beta-amyloid protein
18:43 |
Medical breakthroughs
Dr. George G. Glenner
Congophilic microangiopathy,
Isolation and purification of amyloid protein
Alzheimer's disease and Down's syndrome
Beta amyloid
Mutation of the amyloid precursor protein (APP)
Processing of the APP
Origin of plaques of Alzheimer's, Alan B. McDonald
22:45 |
Potential treatment strategies
EPIX sudy
Amyloid labeling
AVID study
27:00 |
Bedside observations
Patients showed a preference for sweets
29:24 |
University of Pennsylvania scratch-and-sniff Alzheimer's test
Prepiriform cortex (PPC) connectivity
Density of neurofibrillary tangles and senile plaques
Test procedure
35:43 |
Biochemical and neurochemical changes
Reduction of Acetylcholine (ACh)
36:56 |
First treatments for Alzheimer's
Tacrine
Donepezil
Rivastigmine
Memantine
Dimebon study
Animal models
Acetylcholinesterase
Butyrylcholinesterase
44:58 |
Genetics
Types of genes
Mutational genes
Risk factor genes
Apolipoprotein E (APOE)
Relationship with cholesterol
Inflamation, immunoregulation and regeneration
Head trauma
APOE and Alzheimer's disease
ApoE2
ApoE4
Distribution
49:53 |
Non-pharmacologic approaches to Alzheimer's disease
Lifestyle
Caloric restriction (CR)
Mice study
Intermittent fasting, Dr. Mark P. Mattson
Clinical findings in overweight adult asthmatics
Caloric restriction and longevity
Mitohormesis
Insulin signaling
Free radical
Transgenic mouse model
Importance of genes, lifestyle and environment
Physical and mental exercises
Nutrition
Neuron stimulation
Environmental stimulation
Violent patients
Sundowning
Prescribing psychopharmacologic agents
Fear of shadows
59:04 |
Future research
Application of research data to diagnosis and therapy
Understanding mechanisms that lead to Alzheimer's
Cognitive reserve
Educational level
Beta amyloid
Synapses
Neuroglobin
Passive immunization
Tau protein
Alteration of cell cycle and cell death
Removing Tau gene in animals
Alzheimer's and other neurodegenerative diseases
Alzheimer's and normal aging process
Oxidative stress
Tumor necrosis factor
Neurogenesis
Future treatment
Study of neurologic diseases
Summary of studies at Barrow Neurological Institute (BNI)
01:10:31.5 |
Final words
01:10:57.80000000000018 |
Question and answer period
To what extent should doctors reduce cholesterol levels in their patients?
Could you explain mitohormesis?
Is it possible that the lack of excessive food in African countries helps reduce the incidence of dementia?
Is there any difference between the three cholinesterase inhibitors?
Is there any possibility for Guatemalan neurologists to be involved in some of the studies conducted at Barrow Neurological Institute?
Alzheimer’s Disease: “Past, Present and Future” for Physicians
|
04 de febrero de 2009 |
Vistas: 474
In this conference for faculty members of Universidad Francisco Marroquín School of Medicine, Patricio Reyes talks about the history, latest treatment protocols, and most recent research in Alzheimer's disease. Reyes explains the differential diagnosis, key symptoms, early signs of dementia, and changes in brain structure that characterize this disease. He also describes important medical breakthroughs, such as the process of amyloid protein isolation and purification by doctors George G. Glenner and Cai'ne W. Wong, as well as the identification of large numbers of people with Down’s syndrome that also develop Alzheimer’s disease. Nonpharmacological approaches are also discussed.